Gastrointestinal stromal tumor (GIST) is most common
Others include lipoma, carcinoid, leiomyoblastoma, lymphangioma, neural tumors
IMAGING
• Upper GI series: Intact mucosa, obtuse or right angles with wall
• GIST: Often large with central necrosis and ulceration of overlying mucosa on CT
Central area of low attenuation (hemorrhage, necrosis, or cystic formation)
Most GIST > 2 cm have necrosis ± cavitation
• Lipoma: Most common in antrum
May prolapse through pylorus into duodenum
Well-circumscribed areas of uniform fat density = definitive diagnosis
TOP DIFFERENTIAL DIAGNOSES
• Gastric carcinoma
• Gastric metastases and lymphoma
• Ectopic pancreatic tissue
• Pancreatic pseudocyst
• Splenosis
• Gastric ulcer
• Hematoma/seroma
CLINICAL ISSUES
• Carcinoid tumors may be multiple as a result of excess gastrin secretion (Zollinger-Ellison syndrome or atrophic gastritis)
DIAGNOSTIC CHECKLIST
• Lipomas have pathognomonic CT appearance
• GIST has characteristic appearance, but other tumors have overlapping features
• Isolated gastric target lesion is usually GIST
• Multiple target lesions are usually due to metastases
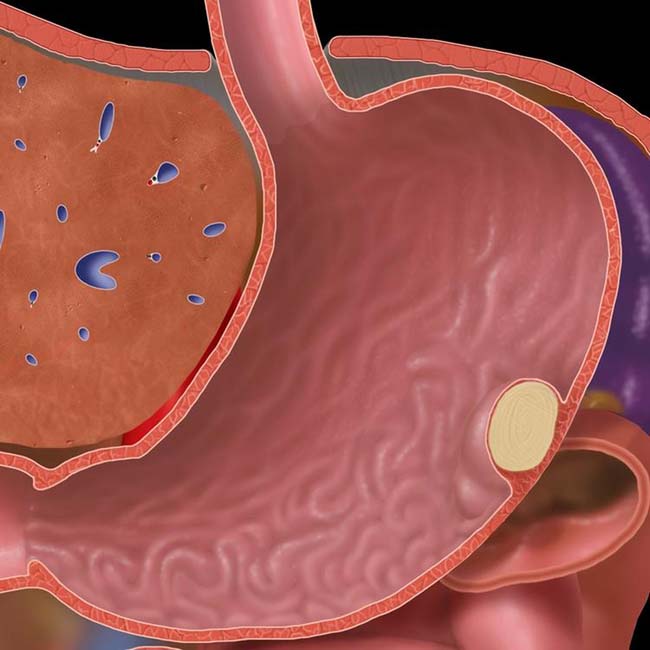
(Left) Graphic shows a “generic” intramural gastric mass with intact mucosa and slightly obtuse or right angles at the interface with the gastric wall.
(Right) Axial CECT shows a discrete fat-density mass within the gastric wall with intact, stretched mucosa; diagnostic of a lipoma.
(Left) Upper GI series shows a gastric antral mass with a central ulceration , typical of a gastric gastrointestinal stromal tumor (GIST). Note the otherwise intact mucosa over the mass, even with preservation of the areae gastricae.
(Right) Endoscopic photograph in the same patient shows the submucosal benign gastric GIST with central ulceration .
TERMINOLOGY
Definitions
• Benign mass composed of 1 or more tissue elements of gastric wall
IMAGING
General Features
• Best diagnostic clue
Intramural mass with smooth surface and slightly obtuse borders







 within the gastric wall with intact, stretched mucosa; diagnostic of a lipoma.
within the gastric wall with intact, stretched mucosa; diagnostic of a lipoma.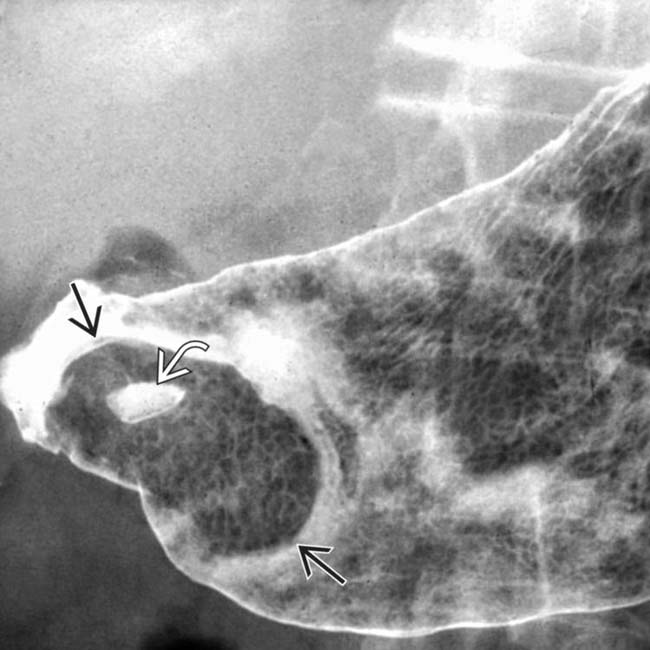
 with a central ulceration
with a central ulceration  , typical of a gastric gastrointestinal stromal tumor (GIST). Note the otherwise intact mucosa over the mass, even with preservation of the areae gastricae.
, typical of a gastric gastrointestinal stromal tumor (GIST). Note the otherwise intact mucosa over the mass, even with preservation of the areae gastricae.
 with central ulceration
with central ulceration  .
.



























