10
Kidney
Renal Cyst
Overview
 Usually benign and found in population over the age of 50 years
Usually benign and found in population over the age of 50 years
Signs and Symptoms
 Usually asymptomatic and incidentally found on imaging
Usually asymptomatic and incidentally found on imaging
Diagnosis
 CT, ultrasound, or MRI
CT, ultrasound, or MRI
Treatment
 Majority do not require treatment
Majority do not require treatment
 Percutaneous drainage for symptomatic benign cysts
Percutaneous drainage for symptomatic benign cysts
 Partial or total nephrectomy for complex cystic lesions suspicious of malignancy
Partial or total nephrectomy for complex cystic lesions suspicious of malignancy
The Bosniak Classification for Renal Cysts
 Category I Simple cyst without septa, calcifications, or solid components. Cyst does not enhance on imaging. Risk of malignancy 0% to <2%
Category I Simple cyst without septa, calcifications, or solid components. Cyst does not enhance on imaging. Risk of malignancy 0% to <2%
 Category II Cyst with a few thin septa. There might be presence of fine calcifications within the septa or wall. Cysts are <3 cm in size, well marginated. Cyst does not enhance on imaging. Risk of malignancy 13%
Category II Cyst with a few thin septa. There might be presence of fine calcifications within the septa or wall. Cysts are <3 cm in size, well marginated. Cyst does not enhance on imaging. Risk of malignancy 13%
 Category IIF Cyst may contain more thin septa but the septa or wall does not enhance on imaging. Cyst might contain thicker or even nodular calcifications that does not enhance on imaging. There are no enhancing soft tissue elements. Lesions that are intrarenal, measuring ≥3 cm without enhancement on imaging are also included in this category. Risk of malignancy 14% to 24%
Category IIF Cyst may contain more thin septa but the septa or wall does not enhance on imaging. Cyst might contain thicker or even nodular calcifications that does not enhance on imaging. There are no enhancing soft tissue elements. Lesions that are intrarenal, measuring ≥3 cm without enhancement on imaging are also included in this category. Risk of malignancy 14% to 24%
 Category III Indeterminate cystic lesions with thickened, irregular wall or septa. Positive enhancement on imaging. Risk of malignancy 50%
Category III Indeterminate cystic lesions with thickened, irregular wall or septa. Positive enhancement on imaging. Risk of malignancy 50%
 Category IV Complex cystic lesions that have all the characteristics under category III. Also, the lesion has adjacent enhancing soft tissue component which is independent of the wall or septa. Risk of malignancy 90%
Category IV Complex cystic lesions that have all the characteristics under category III. Also, the lesion has adjacent enhancing soft tissue component which is independent of the wall or septa. Risk of malignancy 90%
RADIOLOGY
 US findings
US findings
• Anechoic, well-defined masses, with thin walls and posterior acoustic enhancement
 CT findings (Fig. 10.1)
CT findings (Fig. 10.1)
• Well-defined rounded mass with low attenuation values of 0 to 20 HU
• Well defined walls with or without septae (refer to Bosniak classification)
• No internal enhancement on post contrast images
 MRI findings
MRI findings
• Well defined lesion usually with low signal intensity on T1-weighted images if it contains simple fluid, or higher signal intensity if it contains blood
• Uniformly hyperintense on T2-weighted images
• No internal enhancement after contrast medium administration
FIGURE 10.1 A–C
A. Vertebra
B. Descending aorta
C. IVC
D. Small bowel loops
E. Liver
F. Stomach
G. Spleen
H. Psoas muscle

FIGURE 10.1 A
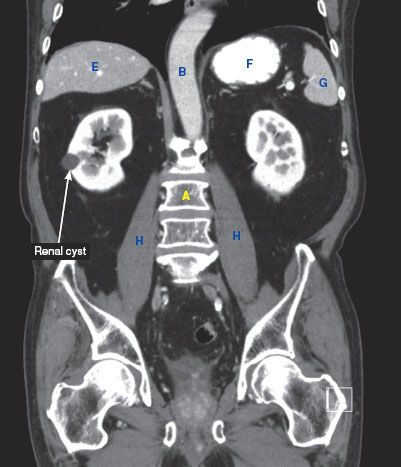
FIGURE 10.1 B

FIGURE 10.1 C
Renal Cell Carcinoma
Overview
 Most common kidney cancer in the adult population
Most common kidney cancer in the adult population
 Most are found incidentally on radiology imaging
Most are found incidentally on radiology imaging
 Most common in men ages 50 to 70 years of age
Most common in men ages 50 to 70 years of age
 Risk factors include smoking and obesity
Risk factors include smoking and obesity
Clinical Presentation
 Flank pain, hematuria, palpable flank mass (10% of patients have this triad)
Flank pain, hematuria, palpable flank mass (10% of patients have this triad)
 Weight loss
Weight loss
 Common sites of metastasis are lung, bone, and liver
Common sites of metastasis are lung, bone, and liver
Diagnosis
 Obtain a noncontrast study and a contrast study to look for increased enhancement of the mass after injection of contrast
Obtain a noncontrast study and a contrast study to look for increased enhancement of the mass after injection of contrast
 If patient cannot receive contrast, consider an MRI with gadolinium, if GFR (glomerular filtration rate) > 30
If patient cannot receive contrast, consider an MRI with gadolinium, if GFR (glomerular filtration rate) > 30
 CXR or Chest CT to rule out metastasis
CXR or Chest CT to rule out metastasis
Treatment
 After appropriate staging is made, then perform radical or partial nephrectomy depending on the size or location of the tumor
After appropriate staging is made, then perform radical or partial nephrectomy depending on the size or location of the tumor
 Possibly requires immunotherapy such as interleukin-2 or interferon alpha
Possibly requires immunotherapy such as interleukin-2 or interferon alpha
RADIOLOGY
 Plain film findings
Plain film findings
• Often normal unless mass is large or contains calcification
• Mass effects on nearby organs may be seen if tumor is very large
 CT findings (Fig. 10.2)
CT findings (Fig. 10.2)
• Enhancement pattern may be heterogeneous due to the presence of hemorrhage and/or necrosis
• Detection of small hypervascular RCC masses is optimal in the corticomedullary or nephrographic phase
• RCC usually shows a lobular margin with adjacent normal tissue but can sometimes infiltrate calyces or the renal pelvis
• Tumor spread through the renal veins and into the IVC may warrant cardiopulmonary bypass if tumor resection is elected
 MRI findings
MRI findings
• Renal cell carcinomas demonstrate contrast enhancement on T1-weight images, and variable signal characteristics on T2-weighted images
FIGURE 10.2 A,B
A. Kidney
B. Vertebra
C. Descending aorta
D. IVC
E. Transverse colon
F. Small bowel loops
G. Liver
H. Stomach
I. Spleen
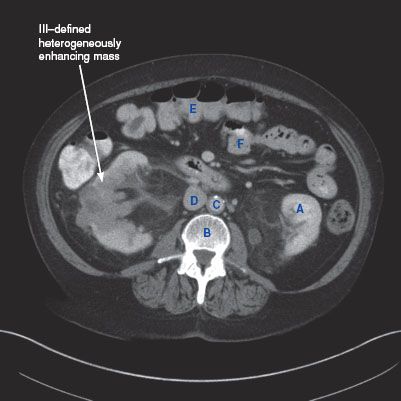
FIGURE 10.2 A




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


