Case presentation
A 9-year-old female presents with 5 weeks of progressively worsening left knee pain. There has been no known trauma and the family denies fever, rash, knee swelling or erythema, weakness, numbness, or incontinence. She is able to ambulate but, due to her pain, has been excused from physical education classes at school. She has seen numerous physicians, and multiple plain radiographs of the left knee were reported as “normal” according to the family. Her primary care provider obtained bloodwork (a complete blood count, erythrocyte sedimentation rate, and C-reactive protein), and the family was told this also was “normal.”
The child is afebrile and has normal, age-appropriate vital signs; her weight is 60 kg, with a height of 142 cm (body mass index of 22.5). Her examination shows a child who is not in distress until you ask her to ambulate. She complies and you notice a demonstrable limp to her left side. Her pelvis is stable and unremarkable. Your examination does not show any signs of trauma and there is no edema, erythema, warmth, or tenderness of her left knee. You perform range-of-motion maneuvers of the knee, which are normal. You examine her left thigh, which also appears unremarkable. Range of motion of her left leg at the hip produces knee pain and mild left hip pain. Her lower leg examination, including her ankle and foot, is unremarkable, including distal pulses. She has no cervical, thoracic, or lumbar findings. Her neurologic examination is nonfocal; she has equal strength of her lower extremities.
Imaging considerations
Plain radiography
Plain radiography is the initial imaging modality of choice for most pediatric orthopedic complaints and remains the initial modality of choice for slipped capital femoral epiphysis (SCFE). The exposure to ionizing radiation is minimal, sedation is not required, and plain radiography is widely available. Proper technique is essential. For suspected hip pathology, pediatric plain radiographs of the pelvis should include anteroposterior (AP) and frog leg lateral views. , Signs of SCFE on plain radiography include posterior and medial slippage of the femoral head, decreased craniocaudal height of the femoral head, evidence of posterior lip of the epiphysis superimposed on the metaphysis, widening and irregularity of the growth plate, and an abnormal relationship of the lateral femoral head to the Klein line. , The Klein line is drawn along the superolateral border of the femoral neck and should intersect the lateral proximal femoral epiphysis. Although the Klein line can be used to detect slippage, recent studies have called into question the utility of this line, especially in subtle SCFE or cases of preslippage. ,
It is not adequate to obtain a hemipelvis view in pediatric patients, as both femoral heads and the complete pelvis should be visualized. Subtle findings of SCFE, Legg-Calve-Perthes disease, or other pathology can be overlooked if only a hemipelvis view is utilized. Evaluation of the contralateral hip is also indicated as bilateral SCFE is common and occurs in greater frequency in patients with endocrine disorders, who have a higher incidence of SCFE. , If a patient cannot perform the frog lateral view due to pain, cross-table lateral views can be obtained. The role of other imaging modalities is controversial and generally indicated on an individual case basis. Options include the following.
Ultrasound (US)
The utilization of sonography for pediatric musculoskeletal complaints has risen in recent years. This modality has been well established in the detection of developmental dysplasia of the hip and is the imaging modality of choice for these patients. , , The use of US for the detection of SCFE has been described previously with a reported accuracy of 93%. , , Common findings of SCFE on US include displacement of the proximal femoral epiphysis compared to the metaphysis, referred to as a physeal step-off, and joint effusion. ,
US for SCFE has the advantage of avoiding ionizing radiation, but expertise in specialized pediatric orthopedic US is required to produce meaningful images and provide correct interpretation. Therefore, at this time, US evaluation for SCFE is not widely available.
Magnetic resonance imaging (MRI)
Without the use of ionizing radiation, MRI can detect early SCFE, prior to anatomic slippage of the femoral head. Additionally, MRI has the advantage of detecting other pathology, especially inflammatory processes and avascular necrosis. MRI is also used as an adjunctive test, after treatment for SCFE, to monitor disease progression or complications, especially the development of avascular necrosis of the femoral head. Limitations include institutional availability and the need for possible sedation.
Computed tomography (CT)
CT is not an initial imaging modality of choice but may be used for pre- or postoperative planning. , Proximal femoral deformities can be evaluated, assisting in osteotomy if indicated. Postoperative intra-articular penetration of femoral hardware can also be assessed with CT. , A limiting factor in its use is exposure to ionizing radiation.
Imaging findings
In this patient, one could repeat films of the knee (AP, lateral, and a patellar view). This may be appropriate if access to the prior images or their interpretation is not available, or if there are concerning physical examination findings that warrant repeat imaging of the knee. However, physical examination elicited primarily left hip pain, with radiation to the left upper knee. In light of the history and physical examination findings, plain radiography of the pelvis is indicated, including AP and frog leg views.
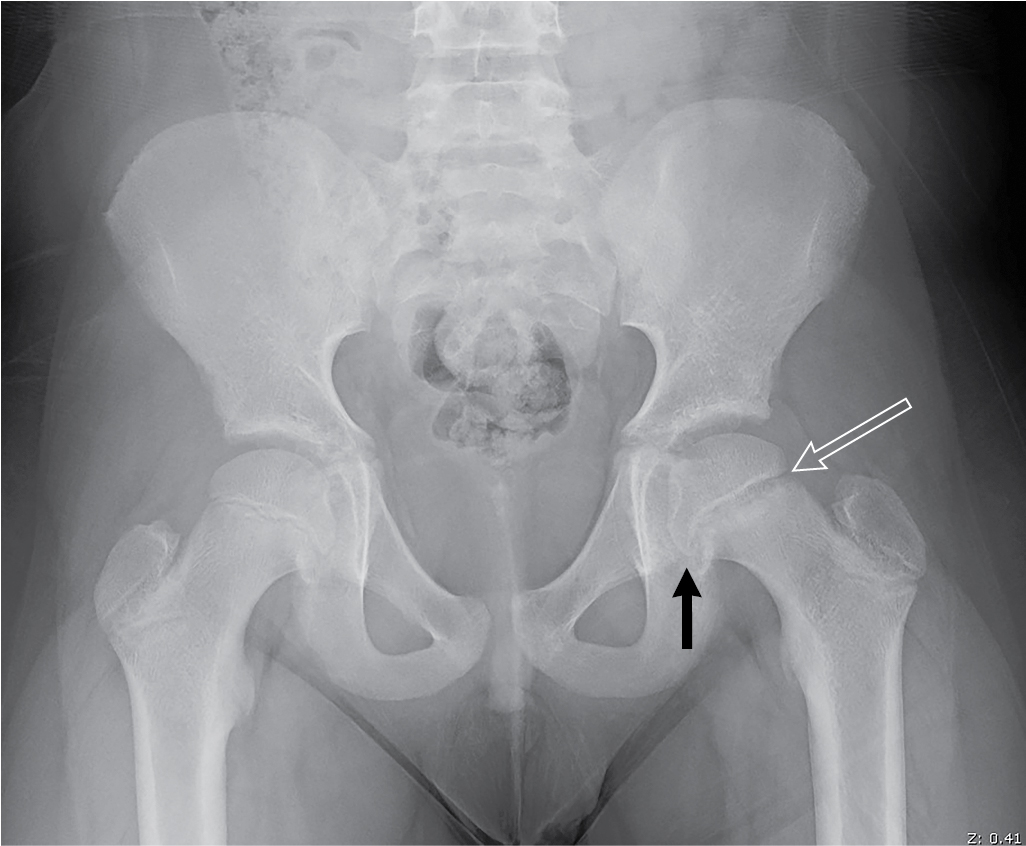
There is widening and irregularity of the left proximal femoral physis, with mild posterior and medial slippage of the left proximal femoral epiphysis, best visualized on the frog leg view ( Figs. 65.1 and 65.2 ). These findings are consistent with SCFE. A useful method to detect the presence of an SCFE is the Klein line. This is a line drawn along the superior edge of the neck of the femur. This line should intersect the lateral portion of the superior femoral epiphysis ( Fig. 65.3 ).