38 Lateral Femoral Cutaneous Nerve Block
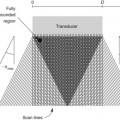
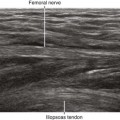
High-resolution ultrasound imaging can identify the LFCN superficial to the sartorius muscle in the proximal thigh.1,2 The nerve has a characteristic medial to lateral course over this muscle. The nerve and muscle are best visualized just medial and distal to the ASIS. As with other small nerves, it is necessary to scan along the length of the nerve to confirm nerve identity. The best imaging technique is to slide the transducer along the known course of the nerve with the nerve viewed in short axis. LFCNs that pass through the sartorius are easier to image because the nerve is surrounded by hypoechoic muscle that provides better acoustic contrast than echobright subcutaneous tissue. Although ultrasound imaging of the LFCN has been reported, the nerve is normally small (1-3 mm in diameter), and sonographic visualization can be difficult within the echobright subcutaneous tissue of the anterior thigh.
LFCN block can be used alone or in conjunction with other lower extremity blocks. It is useful for skin graft harvests and surgical procedures with lateral incisions of the thigh. It is one of the few lower extremity blocks for weight-bearing patients (this group also includes ankle block and saphenous block). LFCN block can improve thigh tourniquet tolerance when combined with other lower extremity blocks.3
Ultrasound imaging may be useful for the diagnosis and treatment of meralgia paresthetica (from Greek meros for “thigh,” and algos for “pain”). Meralgia can result from mechanical stretch or compression injury of the LFCN. Abnormal nerve morphology has been described in patients with meralgia paresthetica. Fusiform enlargement of the LFCN, loss of fascicular discrimination, and hyperemia can all occur in this condition.4–6