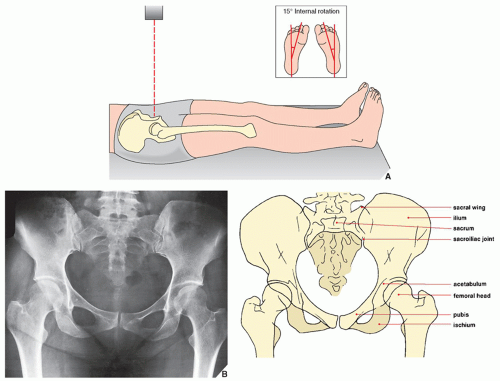
 FIGURE 8.1 Anteroposterior view. (A) For the anteroposterior view of the pelvis and hip, the patient is supine with the feet in slight (15 degrees) internal rotation (inset), which compensates for the normal anteversion of the femoral neck (see Fig. 8.7B), elongating its image. For a view of the entire pelvis, the central beam is directed vertically toward the midportion of the pelvis; for selective examination of either hip joint, it is directed toward the affected femoral head. (B) The radiograph in this projection demonstrates the iliac bones, the sacrum, the pubis, and the ischium, as well as the femoral heads and necks and both the greater and the lesser trochanters. The acetabula are partially obscured by the overlying femoral heads, and the sacroiliac joints are seen en face. |
 FIGURE 8.2 Femoral shaft and neck angles. (A) The angle formed by the longitudinal axes of the femoral shaft and neck normally ranges from 125 to 135 degrees. In the evaluation of displacement in femoral neck fractures, a decrease in this angle (B) is known as a varus deformity, while an increase (C) characterizes a valgus deformity. |
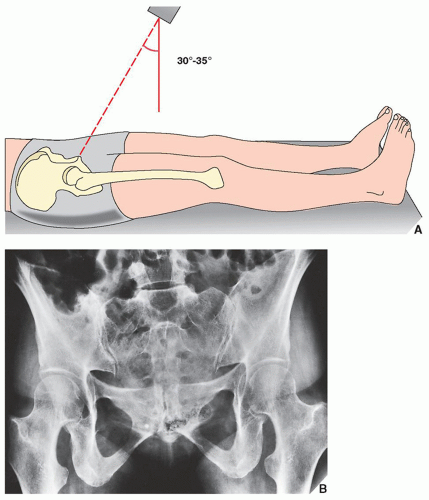 FIGURE 8.3 Ferguson view. (A) For the angled anteroposterior (Ferguson) view of the pelvis, the patient is in the same position as for the standard anteroposterior projection. The radiographic tube, however, is angled approximately 30 to 35 degrees cephalad, and the central beam is directed toward the midportion of the pelvis. (B) The radiograph in this projection provides a tangential view of the sacroiliac joints and the sacral bone. The pubic and ischial rami are also well demonstrated. |
 FIGURE 8.4 Anterior oblique view. (A) For the anterior oblique (Judet) view of the pelvis, the patient is supine and anteriorly rotated, with the affected hip elevated 45 degrees (inset). The central beam is directed vertically toward the affected hip. (B) On the radiograph in this projection, the iliopubic (anterior) column (arrows) (see Fig. 8.20) and the posterior lip (rim) of the acetabulum (open arrow) are well delineated. |
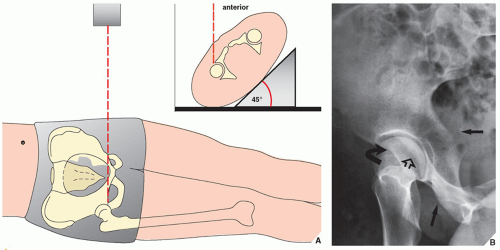 FIGURE 8.5 Posterior oblique view. (A) For the posterior oblique (Judet) view of the pelvis, the patient is supine and anteriorly rotated, with the unaffected hip elevated 45 degrees (inset). The central beam is directed vertically through the affected hip. (B) On the radiograph obtained in this projection, the ilioischial (posterior) column (arrows), the posterior acetabular lip (open arrow), and the anterior acetabular rim (curved arrow) are well demonstrated (see Fig. 8.20). |
 FIGURE 8.6 Frog-lateral view. (A) For the frog-lateral view of the proximal femur and hip, the patient is supine with the knees flexed, the soles of the feet together, and the thighs maximally abducted. For simultaneous imaging of both hips, the central beam is directed vertically or with 10 to 15 degrees cephalad angulation to a point slightly above the pubic symphysis (inset); for selective examination of one hip, it is directed toward the affected hip joint. (B) The radiograph obtained in this projection demonstrates the lateral aspect of the femoral head and both trochanters. |
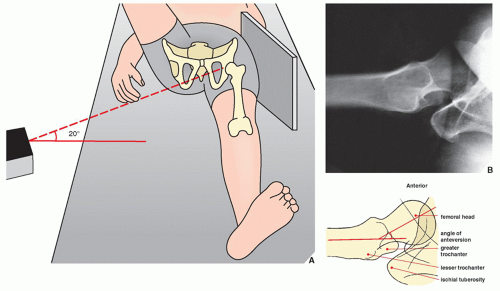 FIGURE 8.7 Groin-lateral view. (A) For the groin-lateral view of the hip, the patient is supine with the affected extremity extended and the opposite leg elevated and abducted. The cassette is placed against the affected hip on the lateral aspect, and the central beam is directed horizontally toward the groin with approximately 20 degrees cephalad angulation. (B) The radiograph obtained in this projection provides almost a true lateral image of the femoral head, thereby allowing evaluation of its anterior and posterior aspects. It also demonstrates the anteversion of the femoral neck, which normally ranges from 25 to 30 degrees. |
 FIGURE 8.8 CT of the sacroiliac and hip joints. (A) CT section at the level of S2 demonstrates the true (synovial) sacroiliac joints. (B) In this section through the hip joints, the relation of the femoral heads to the acetabula can be evaluated sufficiently. The pubic bone and the pubic symphysis are also well delineated. |
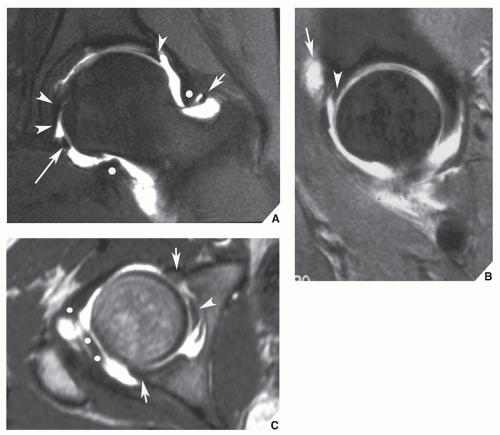 FIGURE 8.9 Normal MRa of the hip. (A) Coronal T1-weighted fat-saturated MRa demonstrates the normal superior labrum (single arrowhead), the ligamentum teres (double arrowheads), the orbicular zone (white dots), the transverse ligament (long arrow), and the superior retinaculum (short arrow). (B) Sagittal T1-weighted fat-saturated MRa demonstrates the superior labrum (arrowhead) and a small amount of contrast material in the iliopsoas bursa (arrow), a feature seen in about 15% of the normal population. (C) Axial T1-weighted MRa demonstrates the ligamentum teres (arrowhead), the orbicular zone (white dots), and the anterior and posterior labrum (arrows). |
TABLE 8.1 Standard and Special Radiographic Projections for Evaluating Injury to the Pelvis, Acetabulum, Sacrum, and Proximal Femur | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 8.2 Ancillary Imaging Techniques for Evaluating Injury to the Pelvis, Acetabulum, and Proximal Femur | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
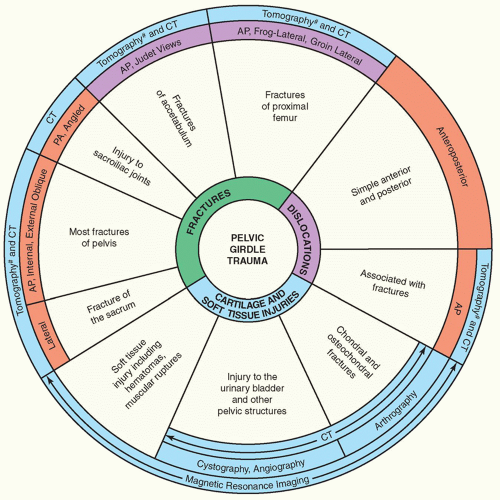 FIGURE 8.10 Spectrum of radiologic imaging techniques for evaluating injury to the pelvic girdle. The radiographic projections or radiologic techniques indicated throughout the diagram are only those that are the most effective in demonstrating the respective traumatic conditions. #Replaced almost completely by CT. CT, computed tomography; AP, anteroposterior. |
 FIGURE 8.11 Stable pelvic fractures. (Modified from Dunn AW, Morris HD. Fractures and dislocations of the pelvis. J Bone Joint Surg [Am] 1968;50A:1639-1648.) |
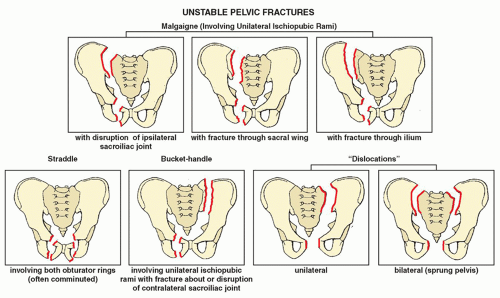 FIGURE 8.12 Unstable pelvic fractures. (Modified from Dunn AW, Morris HD. Fractures and dislocations of the pelvis. J Bone Joint Surg [Am] 1968;50A:1639-1648.) |
pelvic injuries. They identified four patterns of force as underlying mechanisms of injury that produce distinctive radiographic appearances:
Anteroposterior compression, in which the force vector in the anteroposterior or posteroanterior direction produces vertically oriented fractures of the pubic rami and disruption of the pubic symphysis and sacroiliac joints, which often results in bilateral pelvic “dislocation” (sprung pelvis, “open book” injury).
Lateral compression, in which the lateral force vector often results in horizontally or coronally oriented fractures of the pubic rami, compression fractures of the sacrum, fractures of the iliac wings, and central dislocation in the hip joint as well as varying degrees of pelvic instability caused by displacement or rotation of one or both hemipelves, depending on whether the compressive force is applied more anteriorly or more posteriorly.
Vertical shear, in which the inferosuperiorly oriented disruptive force, delivered to one or both sides of the pelvis lateral to the midline often as a result of a fall from a height, frequently produces vertically oriented fractures of the pubic rami, sacrum, and iliac wings. Because of significant ligamentous disruption, this type of force is associated with injuries producing severe pelvic instability.
Complex patterns, in which at least two different force vectors have been delivered to the pelvis, the patterns produced by anteroposterior and lateral compression being the most commonly encountered.
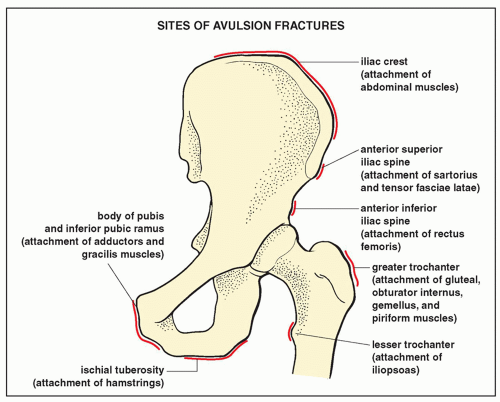 FIGURE 8.13 Sites of avulsion fractures. |
 FIGURE 8.14 Avulsion fractures. A 16-year-old boy was injured during an athletic activity. (A) Anteroposterior radiograph of the pelvis shows a crescent-shaped fragment adjacent to the lateral aspect of the iliac wing (arrow), which represents the avulsed apophysis of the anterosuperior iliac spine. (B) Anteroposterior radiograph of the hip in a 26-year-old runner clearly demonstrates avulsion of the ischial tuberosity. (C) As a sequela of avulsion of the ischial tuberosity and injury to the soft tissue in the region, a 28-year-old athlete had ossification of the obturator externus muscle. |
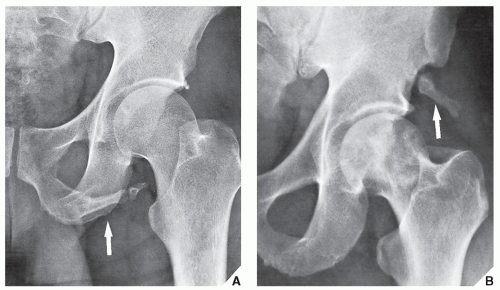 FIGURE 8.15 Pelvic digit. A rare congenital anomaly, the pelvic digit may occasionally be mistaken for avulsion fracture. (A) Anteroposterior radiograph of the left hip shows a finger-like, jointed structure attached to the caudal portion of the left ischium (arrow). (B) Anteroposterior radiograph of the hip in a 55-year-old man with no history of trauma demonstrates a well-formed digit at the site of the anteroinferior iliac spine (arrow). (From Greenspan A, Norman A. The “pelvic digit”—an unusual developmental anomaly. Skeletal Radiol 1982;9:118-122.) |
surrounding structures (Fig. 8.18). Fracture of the acetabulum usually distorts these radiographic landmarks, allowing a diagnosis to be made on the anteroposterior projection, but an accurate and complete evaluation of the fracture requires that oblique views be obtained (Fig. 8.19). As mentioned, the anterior (internal) oblique projection demonstrates the iliopubic column and the posterior lip of the acetabulum (see Fig. 8.4), and the posterior (external) oblique view images the ilioischial column and the anterior rim of the acetabulum (see Fig. 8.5). These projections, together with the division of the pelvic bone into anterior and posterior columns (Fig. 8.20), provide the basis for the traditional classification of acetabular fractures. This classification has been modified by Letournel to include the following types of fractures (Fig. 8.21) :
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


