and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
5.1 Case 1: Staging of Lung Carcinoma
History
A 58-year-old male underwent 18F-FDG PET/CT scan after he was diagnosed to have nonsmall cell lung carcinoma (NSCLC) with a bronchoscopic biopsy.
Findings
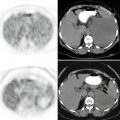
Fig. 5.1
Axial CT and fusion images show intensely hypermetabolic mass lesion (SUVmax 12.9) at right upper lobe adjacent to mediastinum with a hypometabolic necrotic center and another solid lesion located anteriorly with increased FDG uptake (SUVmax 13.9) (a, b), hypermetabolism at the nodular lesion at left surrenal gland (SUVmax8.9) (c, d)
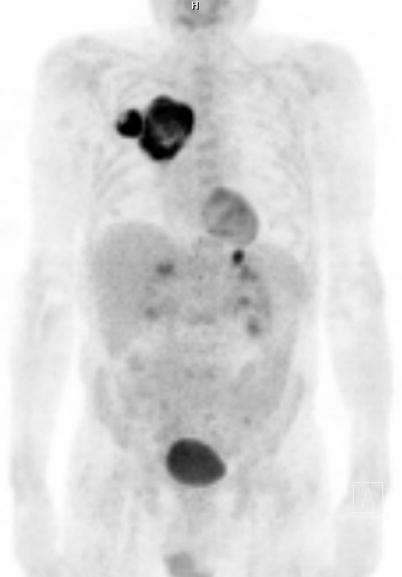
Fig. 5.2
MIP image
Interpretation
Increased uptake at the known primary lesions at right lung and metastatic lesion at left surrenal gland.
Teaching Point
PET detects unsuspected distant metastases in 10 % of patients. Adrenal metastasis, at the initial diagnosis of nonsmall cell lung cancer, occurs in less than 10 % of lung cancer patients. Sensitivity and specificity of PET/CT for adrenal metastasis is 94 % and 85 %, respectively.
5.2 Case 2: Staging of Lung Carcinoma
History
A 55-year-old male with known NSCLC at right lung. The current 18F-FDG PET/CT imaging is being done to evaluate the extent of disease.
Findings
Fig. 5.3
Axial CT and fusion images show intensely hypermetabolic solid lesion (SUVmax 13.6) at right hilus adjacent to the right main bronchus (arrow). There is not any hypermetabolic mediastinal lymph node suspicious for metastatic invasion (a, b). Intensely increased FDG uptake is seen in the lytic lesion at L2 vertebra (arrow) (SUVmax 14) (c, d)
Interpretation
Increased uptake at the primary malignant lesion at right lung and metastatic lesion at L2 vertebra.
Teaching Point
18F-FDG PET/CT is useful in detecting any possible distant metastasis in Stage II, III, and IV.
5.3 Case 3: Staging of Lung Carcinoma
History
A 55-year-old male who was admitted with the complaint of cough was found to have a cavitary lesion at lower lobe of left lung on CT. Bronchoscopic biopsy revealed squamous cell carcinoma of lung (SLC). The current 18F-FDG PET/CT imaging is being done to stage the disease.
Findings
Fig. 5.4
Axial CT and fusion images show hypermetabolic lesion at left lower paratracheal area (SUVmax 10.8) (a, b) and cavitary lesion at left lower lobe with moderately increased FDG uptake (SUVmax 10.6) (c, d)

Fig. 5.5
MIP image
Interpretation
Primary malignant lesion at lower lobe of left lung and metastatic involvement of left lower paratracheal lymph node.
Result
Patient is regarded as Stage IIIA and underwent neoadjuvant chemotherapy before operation.
Teaching Point
If the 18F-FDG PET/CT scan is positive in mediastinum, the lymph node status needs pathological confirmation and mediastinoscopy is done for this purpose.
Cavitating lesions are frequently seen in patients with SLC and these lesions might mimic infectious processes. They are characterized with increased chemoresistance and worse prognosis.
5.4 Case 4: Restaging of Lung Carcinoma
History
A 54-year-old female status post left pneumonectomy for adenocarcinoma of lung underwent 18F-FDG PET/CT imaging for evaluation of the extent of the disease.
Findings
Fig. 5.6
Axial CT and PET images show collapse of left lung due to pneumonectomy and no pathological FDG uptake in favor of local recurrence (a, b) and increased focal FDG uptake at left frontal lobe of brain (SUVmax 10.4) (c, d)

Fig. 5.7
MIP image
Interpretation
Recurrent metastatic lesion at left frontal lobe of brain.
Teaching Point
F-18 FDG PET/CT studies can be done as whole-body imaging; from the top of the head through the feet or torso imaging; base of the skull to mid-thigh. Although torso imaging is usually preferred because of high physiological FDG uptake at brain that can mask metastatic hypermetabolic foci, this case shows the importance of obtaining whole-body imaging when likelihood for metastasis to brain is high.
5.5 Case 5: Detection of Bone Metastasis in Lung Carcinoma
History
A 55-year-old male with NSCLC underwent 18F-FDG PET/CT imaging while being followed-up after having chemotherapy and radiotherapy.
Findings
Fig. 5.8
MIP image (a), axial PET, CT, and fusion images showing focal hyperdense lesion at dorsal vertebras without corresponding FDG uptake (b, c, d) and (e, f, g). Diffuse FDG uptake at upper lobe of right lung represents inflammatory process following radiotherapy
Interpretation
Metastatic sclerotic lesions at corpus of dorsal vertebras.
Teaching Point
18F-FDG PET/CT is less sensitive in detecting sclerotic metastases since they are relatively hypocellular and consequently contain lower volumes of viable tumor tissue causing low degree of uptake of FDG. FDG nonavid osteoblastic lesions can be detected as sclerotic lesions on CT part of the PET/CT studies.
5.6 Case 6: Differentiation of Lung Carcinoma from Atelectasis
History
A 75-year-old female with known right-sided adenocarcinoma. Patient underwent 18F-FDG PET/CT imaging to evaluate the extent of disease.
Findings
Fig. 5.9
Axial PET, CT, and fusion images show increased FDG uptake in the mass lesion at anterior segment of upper lobe of right lung. Anterior to the mass lesion, soft tissue density which exhibits minimally increased FDG uptake on PET image is seen (a–c). Pleural effusion without FDG uptake is also noted at right lung
Interpretation
Compression of the bronchus by the tumor caused atelectasis.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


