and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
7.1 Case 1: Staging of Anaplastic Large Cell Lymphoma
History
A 49-year-old male underwent 18F-FDG PET/CT after having diagnosed as anaplastic lymphoma kinase (ALK) negative anaplastic large cell lymphoma (ALCL) following a biopsy from a lesion located at left inguinal area.
Findings
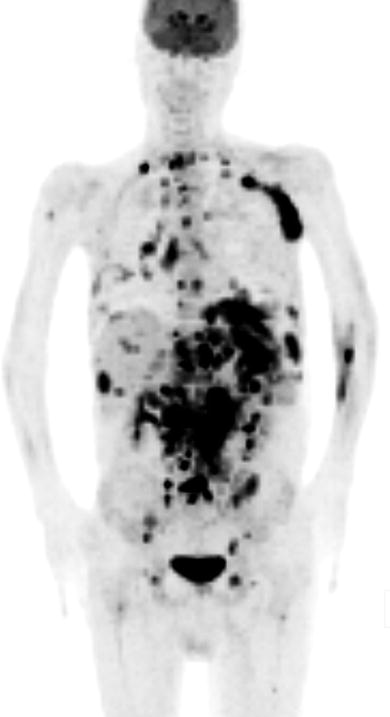
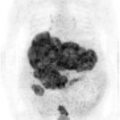
Fig. 7.1
MIP image shows intensely increased FDG uptake at cervical jugular, mediastinal, and intraabdominal lymph nodes (SUVmax 10); hypermetabolic foci at liver and spleen (SUVmax 9); multiple hypermetabolic foci at vertebral colon and pelvic bones
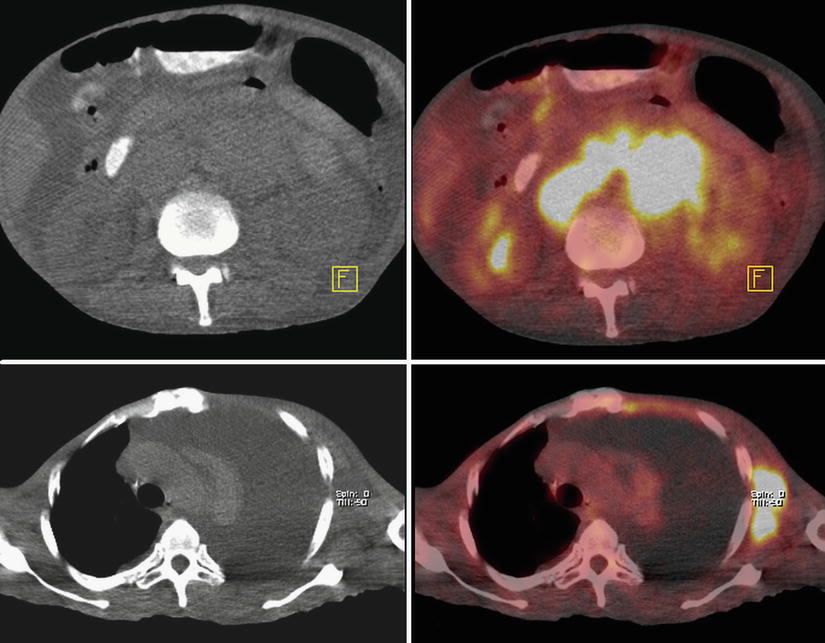
Fig. 7.2
Axial CT and fusion images show intensely hypermetabolic lymph nodes at paraaortic, interaortocaval, and left axillary fossa lymph node stations
Interpretation
Hypermetabolism at lymph nodes, liver, spleen, vertebral colon, and pelvic bones is compatible with multiple metastases.
Teaching Point
ALCL is a rare type of non-Hodgkin lymphoma (NHL). It is divided into two entities according to the expression of ALK. It is an FDG avid malignancy and ALK expression is related to higher FDG uptake. ALK-positive patients tend to have better progression free survival than ALK-negative patients.
7.2 Case 2: Staging of non-Hodgkin Lymphoma
History
A 72-year-old male underwent 18F-FDG PET/CT for pretreatment staging after having diagnosed as NHL with small lymphocytic lymphoma subtype.
Findings

Fig. 7.3
MIP image shows enlargement and diffuse increased FDG uptake (SUVmax 5.2) at spleen. There are also mildly hypermetabolic lymph nodes barely visualized at perigastric, peripancreatic, and bilateral inguinal areas. The spleen/liver SUVmax ratio is 5.2/3

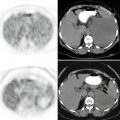
Fig. 7.4
Axial CT and PET images show diffuse hypermetabolism at spleen
Interpretation
Splenomegaly together with increased FDG uptake is consistent with metastatic involvement of spleen. Although FDG uptake is not intense, hypermetabolism at lymph nodes is also suggestive of metastasis.
Teaching Point
18F-FDG PET/CT is an effective method in the evaluation of metastatically involved lymph nodes which are reported as normal on CT depending on the size criterion. It is also superior to CT in the evaluation of diffusely infiltrated sites, such as the spleen or bone marrow. Sensitivity and specificity of PET/CT were higher than those of the other diagnostic modalities alone when the initial staging of splenic lymphomatous involvement is concerned.
7.3 Case 3: Diffuse Large B-Cell Lymphoma
History
A 72-year-old male, status post left axillary lymph node excisional biopsy proven to be Diffuse Large B-Cell Lymphoma (DLBCL) underwent 18F-FDG PET/CT for pretreatment staging.
Findings

Fig. 7.5
MIP image shows hypermetabolic lymph nodes at left axillary fossa; intraabdominal lymph stations; focal hypermetabolic lesion at liver; increased FDG uptake sites at vertebral colon and pelvic bones. Spleen shows enlargement with intense heterogeneous FDG uptake with hypermetabolic foci dispersed through the organ. There is also minimal diffuse hypermetabolism at proximal humeri and both femurs
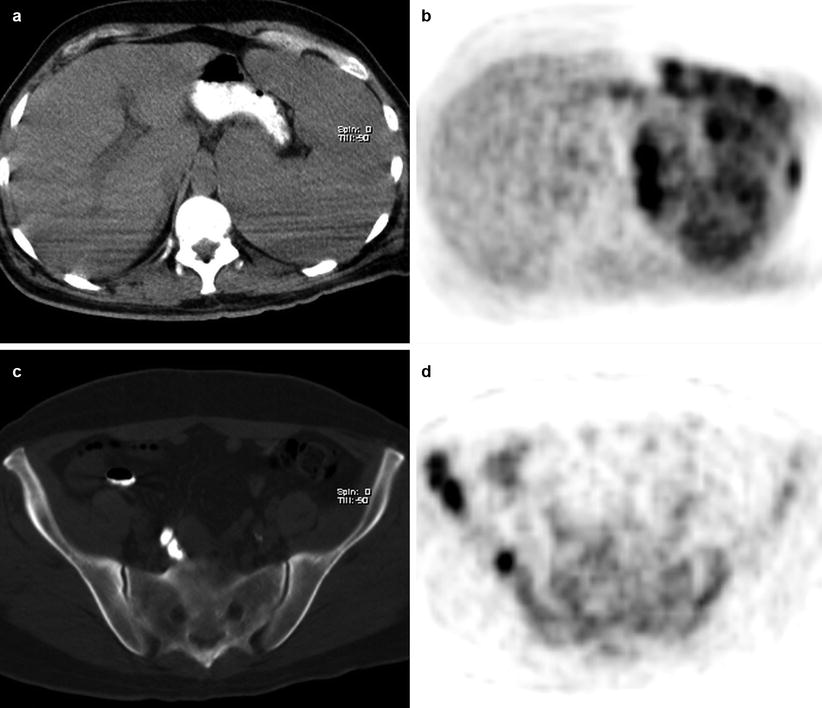
Fig. 7.6
Axial CT and PET images shows hypermetabolic foci disseminated throughout enlarged spleen (a, b) and right iliac wing (c, d)
Interpretation
Increased FDG uptake sites at infra- and supraabdominal lymph node stations, liver, spleen, and bony structures are compatible with metastatic involvement of lymphoma. Diffuse increased bone marrow uptake at proximal humeri and both femurs is due to hematopoietic activation.
Teaching Point
FDG uptake pattern in spleen is heterogenous and multifocal in metastatic infiltration, whereas diffuse and mild in bone marrow activation.
7.4 Case 4: Testicular Lymphoma
History
A 49-year-old male, status post left orchiectomy proven to be DLBCL, underwent 18F-FDG PET/CT scan for pretreatment staging.
Findings
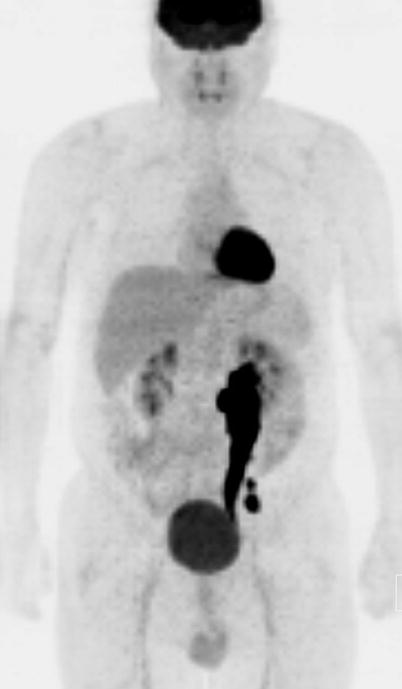
Fig. 7.7
MIP image shows intensely hypermetabolic conglomerate of retroperitoneal lymph nodes at left iliac lymphatic chain (SUVmax 15)

Fig. 7.8
MIP image of study performed 6 months after the patient received chemotherapy and radiotherapy. Lymph nodes with pathological FDG uptake disappeared
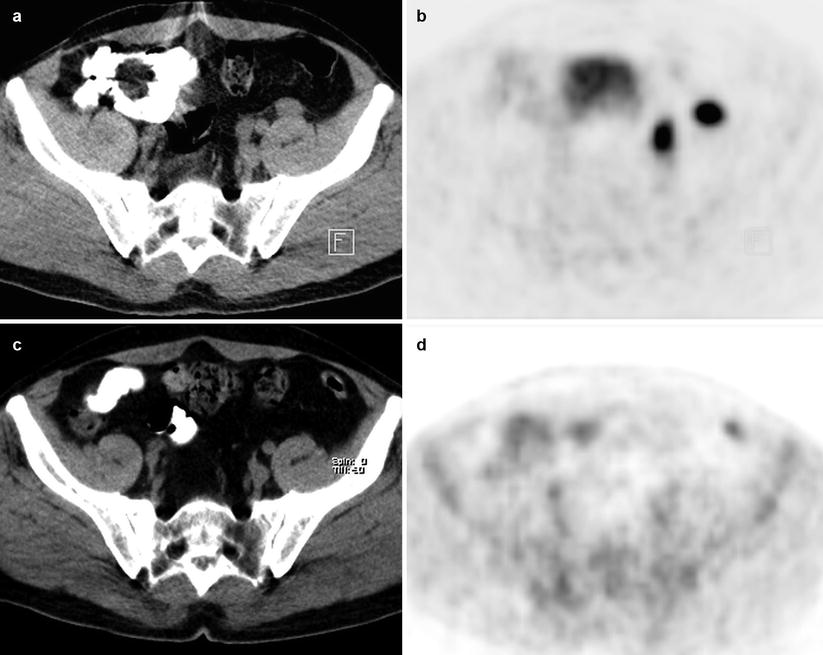
Fig. 7.9
Axial CT and PET images shows hypermetabolic foci at left external iliac region (a, b); resolution of metabolic activity at lymph nodes at PET/CT scan obtained 6 months after the first one (c, d)
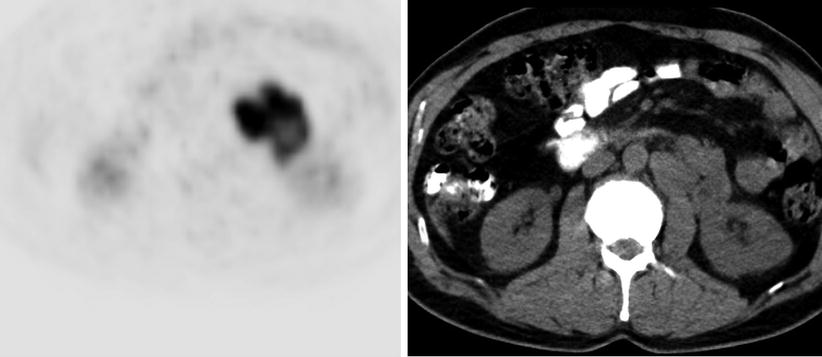
Fig. 7.10
Axial PET and CT images show hypermetabolic foci at left paraaortic region
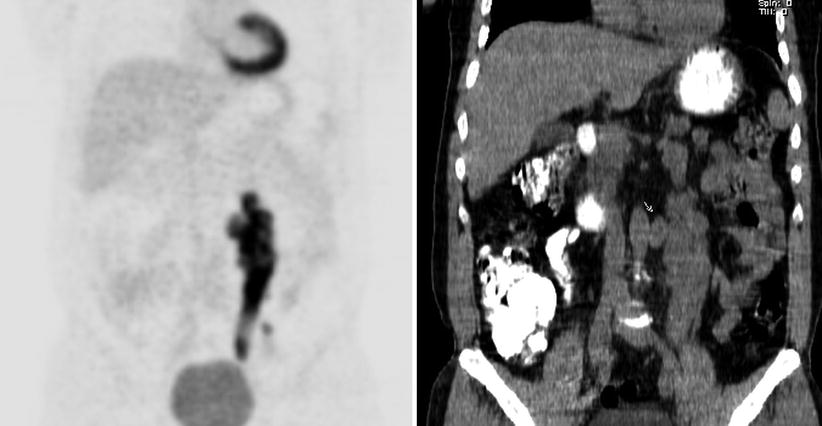
Fig. 7.11
Coronal PET and CT images show hypermetabolic conglomerate retroperitoneal lymph node masses at left iliac lymphatic chain
Interpretation
Hypermetabolic retroperitoneal lymph node masses at left iliac lymphatic chain is compatible with metastatic involvement of lymphoma. The lesions showed complete remission after chemoradiotherapy.
Teaching Point
Primary testicular lymphoma (PTL) comprises around 1–2 % of all NHL. It primarily affects men, with a median age of 67 years. The most common histological subtype is DLBCL, accounting for 80–90 % of PTLs. 18F-FDG PET/CT is currently the standard procedure for assessment of the posttreatment response for most lymphoma subtypes.
7.5 Case 5: Diffuse Large B-Cell Lymphoma Involving Duodenum
History
A 72-year-old male, status post duodenum biopsy proven to be DLBCL, underwent 18F-FDG PET/CT for pretreatment staging.
Findings
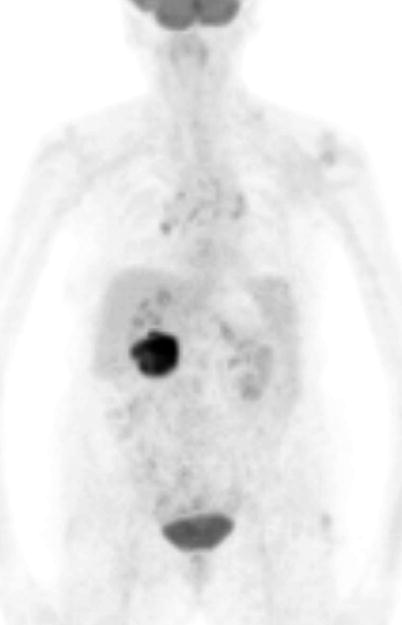
Fig. 7.12
MIP image
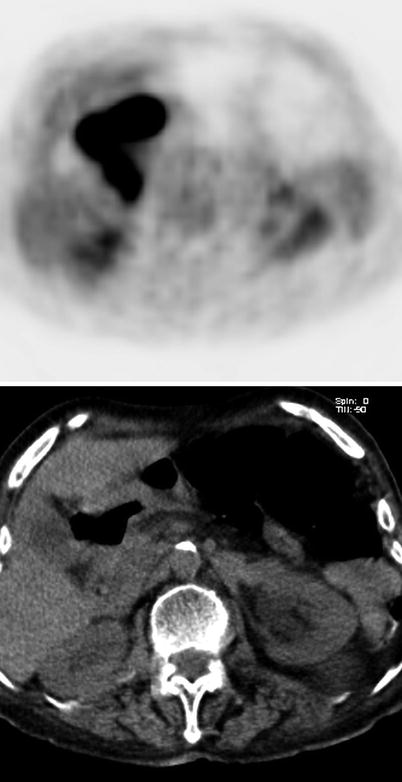
Fig. 7.13
Axial PET and CT images showed intensely increased FDG uptake (SUVmax 25) at duodenum
Interpretation
Hypermetabolism involving the duodenum compatible with extranodal lymphoma.
Teaching Point
Although the GI tract is the predominant site of extranodal lymphomas (ENL), primary lymphomas of the GI tract are rare. 50–60 % of all primary GI lymphomas are NHL. Many of these tumors are of the B-cell type. The duodenum is the most infrequent site of these lesions. 18F-FDG PET-CT has a significant advantage for the diagnosis of diffusely infiltrating organ involvements and is superior to contrast enhanced CT.
7.6 Case 6: Gastric Lymphoma and Virchow’s node
History
A 39-year-old male underwent 18F-FDG PET/CT after having diagnosed as gastric NHL following a biopsy from stomach. PET/CT study was repeated 4.5 months after the patient received chemotherapy and radiotherapy.
Findings
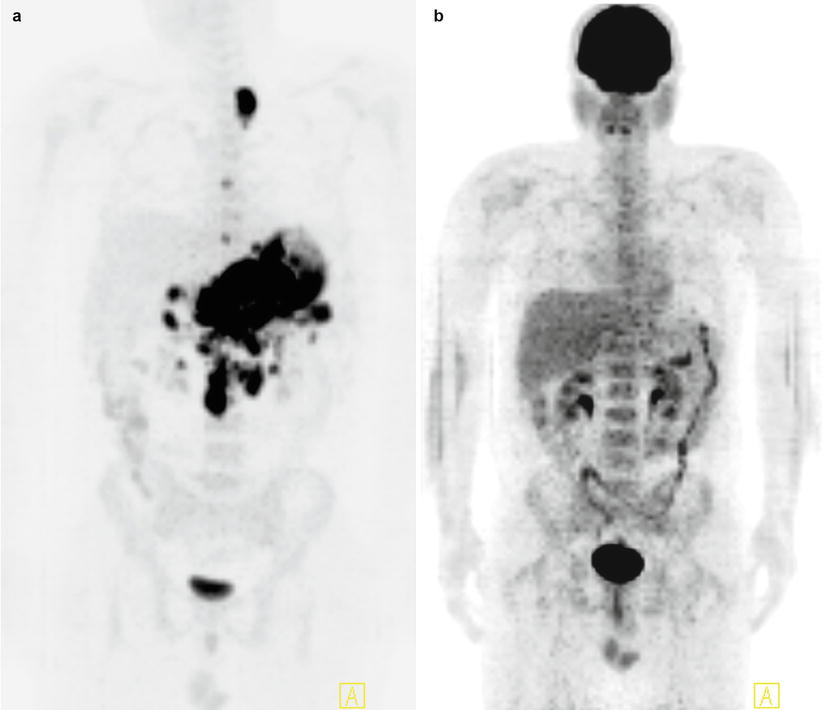
Fig. 7.14
MIP images shows intensely increased FDG uptake at gastric wall (SUVmax 45), numerous hypermetabolic intraabdominal lymph nodes (SUVmax 56) and hypermetabolic lymph node at left supraclavicular area (a), disappearance of all lesions with pathological FDG uptake at study performed 4.5 months after the patient received chemotherapy and radiotherapy (b)
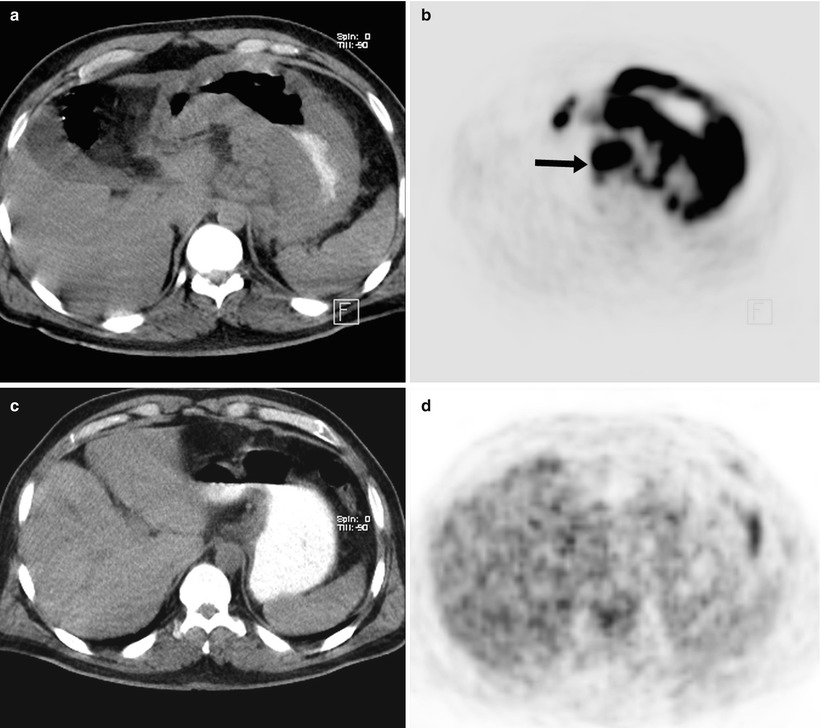
Fig. 7.15
Axial CT and PET images shows highly increased FDG uptake with corresponding abnormal gastric wall thickening and a few perigastric hypermetabolic lymph nodes (arrow) (a, b), resolution of metabolic activity at gastric wall and lymph nodes at 18F-FDG PET CT scan obtained 4.5 months after the first one (c, d)
Fig. 7.16
Axial CT and PET images shows intensely hypermetabolic lymph node at supraclavicular region (arrow) (a, b), resolution of the lesion at the second study (c, d)
Interpretation
Diffuse and intensely increased FDG uptake at gastric wall represents primary malignant disease and hypermetabolic intraabdominal and supraclavicular (Virchow’s node) lymph nodes reflect involvement with primary malignancy. Resolution of all lesions at second study indicates complete remission as a result of chemoradiotherapy.
Teaching Point
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


