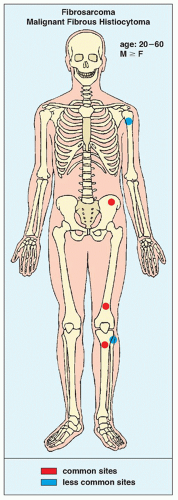
 FIGURE 22.1 Skeletal sites of predilection, peak age range, and male-to-female ratio in fibrosarcoma and MFH. |
 FIGURE 22.2 Fibrosarcoma. Oblique radiograph of the right knee of a 28-year-old woman shows a purely destructive osteolytic lesion in the intercondylar fossa of the distal femur. Note the absence of reactive sclerosis and periosteal response. |
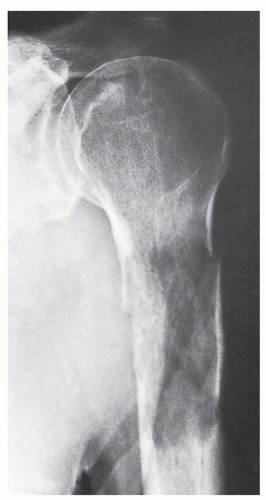 FIGURE 22.3 Fibrosarcoma. A 62-year-old man sustained a pathologic fracture through an osteolytic lesion in the proximal shaft of the left humerus. A metastatic lesion was suspected, but biopsy revealed a primary fibrosarcoma of the bone. |
 FIGURE 22.4 Malignant fibrous histiocytoma. (A) Oblique radiograph of the right femur of a 16-year-old girl shows fusiform thickening of the cortex and permeative type of medullary bone destruction (arrows). (B) Radionuclide bone scan (99mTc-MDP) shows increased uptake of the tracer in the right femur. (C) Coronal T1-weighted (spin echo [SE]; repetition time [TR] 500/echo time [TE] 20 msec) MR image demonstrates the extent of the tumor that involves about 75% of the length of the femur. (D) Coronal T2-weighted (SE; TR 2000/TE 80 msec) MR image shows that the tumor exhibits high signal intensity. The soft-tissue extension medially is also accurately depicted (arrows). |
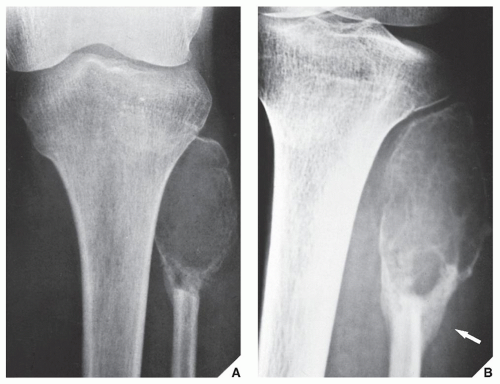 FIGURE 22.5 Malignant fibrous histiocytoma. Anteroposterior radiograph of the left knee (A) and oblique projection (B) demonstrate an expansive, lytic lesion in the proximal end of the fibula in a 13-year-old girl. The cortex has been partially destroyed, and there is a buttress of periosteal new bone formation (arrow) secondary to pathologic fracture. The differential diagnosis of this malignancy at this site should include giant cell tumor and aneurysmal bone cyst. |
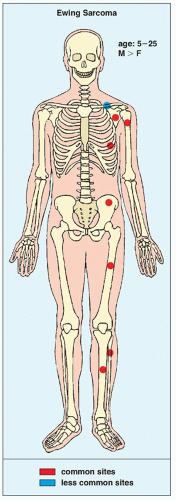 FIGURE 22.6 Skeletal sites of predilection, peak age range, and male-to-female ratio in Ewing sarcoma. |
PNET cannot be made on the basis of radiography. Differentiation between these two tumors must rely entirely on immunohistochemistry, electron microscopy, and molecular genetic studies.
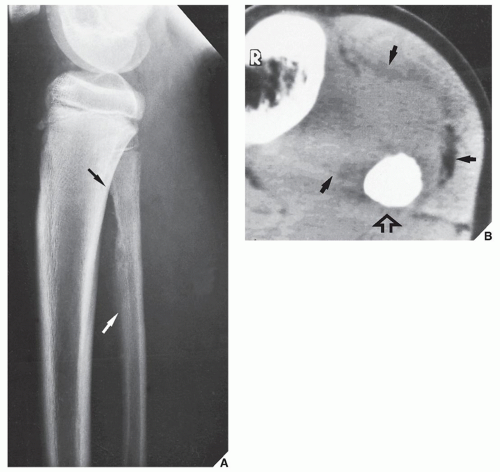 FIGURE 22.7 Ewing sarcoma. (A) Lateral radiograph of a 12-year-old boy shows the typical appearance of this tumor in the fibula. The poorly defined lesion exhibits permeative bone destruction associated with an aggressive periosteal reaction (arrows). (B) CT section through the lesion demonstrates a large soft-tissue mass (arrows), which is not clear on the conventional study. Note the complete obliteration of the marrow cavity by tumor (open arrow). |
 FIGURE 22.8 Ewing sarcoma. (A) Bone destruction (arrow) is almost imperceptible on this radiograph of a 10-year-old girl with tumor in the distal femoral diaphysis. (B) Lateral radiograph of distal femur, however, shows a large soft-tissue mass (arrows). (C) CT using a bone “window” demonstrates destruction of the medullary portion of the bone, endosteal scalloping, and invasion of the cortex. |
 FIGURE 22.9 MRI of Ewing sarcoma. Anteroposterior (A) and lateral (B) radiographs of the right distal femur of a 7-year-old girl show permeative and moth-eaten types of bone destruction in the metaphysis and diaphysis associated with a large soft-tissue mass. Coronal (C) and sagittal (D) T1-weighted (SE; TR 750/TE 20 msec) MR images demonstrate the intraosseous and extraosseous extent of the tumor. (E) Axial T2-weighted (SE; TR 2000/TE 80 msec) MR image shows heterogeneous but mostly high signal intensity of the soft-tissue mass. Note markedly enlarged circumference of the right thigh as compared to the contralateral normal thigh. |
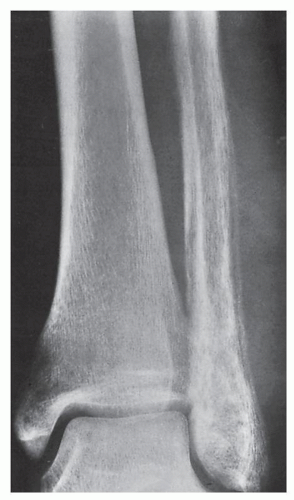 FIGURE 22.10 Ewing sarcoma. A 24-year-old man presented with pain and swelling of the left ankle for 8 weeks; he also had a fever. Anteroposterior radiograph of the ankle demonstrates an aggressive lesion of the distal fibula exhibiting a permeative type of bone destruction and a lamellated periosteal reaction; a soft-tissue mass is also evident. The appearance is that of infection (osteomyelitis), but biopsy confirmed malignancy. |
 FIGURE 22.11 Ewing sarcoma. Anteroposterior radiograph of the right femur of a 12-year-old girl shows “saucerization” of the medial cortex of the diaphysis, often seen in Ewing sarcoma; there is also an associated soft-tissue mass. |
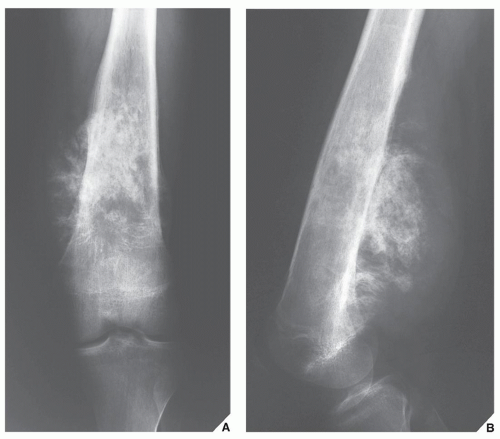 FIGURE 22.12 Ewing sarcoma. Anteroposterior (A) and lateral (B) radiographs of the left femur of a 17-year-old boy show a tumor displaying a significant degree of sclerosis that was originally misinterpreted as osteosarcoma. |
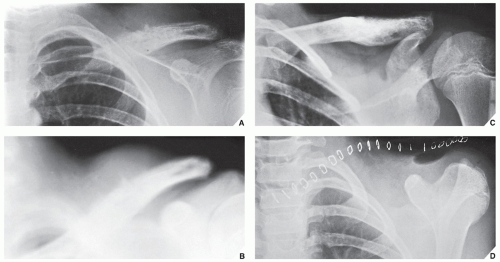 FIGURE 22.13 Treatment of Ewing sarcoma. (A) Radiograph of the shoulder of an 11-year-old boy shows the typical appearance of Ewing sarcoma involving the distal half of the left clavicle. The poorly defined destructive lesion is associated with an aggressive periosteal reaction and a large soft-tissue mass. (B) Tomographic cut gives a better picture of the soft-tissue mass. (C) After a 4-month course of chemotherapy, the lesion has become sclerotic, the periosteal reaction has disappeared, and the soft-tissue mass has shrunk substantially. (D) The clavicle was then removed en bloc. |
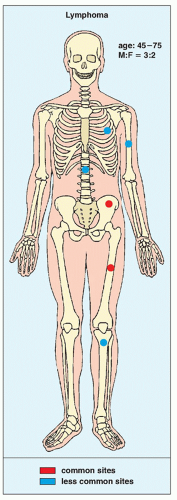 FIGURE 22.14 Skeletal sites of predilection, peak age range, and male-to-female ratio in primary bone lymphoma. |
 FIGURE 22.15 Lymphoma. An 18-year-old woman presented with low back pain for several months, which was attributed to herniation of an intervertebral disk. (A) Myelogram shows that the disk is normal, but the body of L5 (arrow) exhibits a mottled appearance and its posterior border is indistinct. (B) CT section demonstrates a large, osteolytic lesion extending from the anterior to the posterior margins of the vertebral body. |
 FIGURE 22.16 Lymphoma. (A) Anteroposterior radiograph of the pelvis of a 19-year-old woman shows sclerosis of the right ilium (arrows). (B) Axial and (C) coronal reformatted CT images confirm diffuse involvement of the ilium. (D) Total body PET scan shows hypermetabolic tumor involving the right ilium, right ischium, and right-sided sacrum. (Continued) |
 FIGURE 22.16 Lymphoma. Continued (E) Two axial fused FDG PET-CT images confirm the location of the tumor in the ilium, ischium, and sacrum. (F) Axial T1-weighted MR image shows the tumor to be of low signal intensity (arrows). (G) Coronal T1-weighted fat-saturated MR image obtained after intravenous administration of gadolinium demonstrates heterogenous enhancement of the tumor. |
 FIGURE 22.17 CT of Lymphoma. (A) Anteroposterior and oblique radiographs of the right humerus of a 20-year-old man show a long lesion exhibiting permeative and moth-eaten type of bone destruction. Periosteal reaction is secondary to the pathologic fracture. (B) Sagittal reformatted CT image demonstrates endosteal scalloping and early callus formation at the site of a pathologic fracture (arrows). |
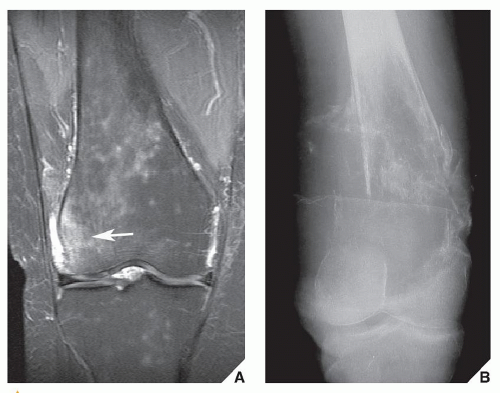 FIGURE 22.18 MRI of lymphoma. (A) Coronal proton density-weighted MRI of a patient with history of trauma shows an ill-defined area of increased signal intensity in the lateral femoral condyle (arrow), originally interpreted as bone contusion. Multiple smaller areas of increased signal intensity noted in the distal femur were interpreted as red marrow islands. (B) Follow-up anteroposterior radiograph of the knee obtained a year later demonstrates a large lytic lesion of the distal femur with a pathologic fracture. |
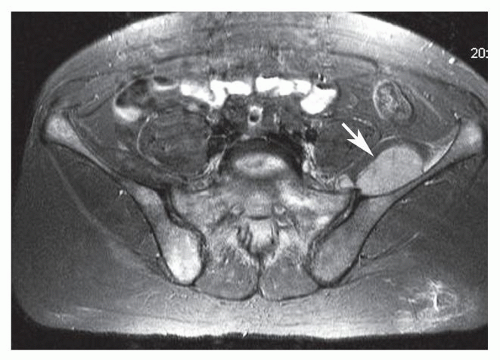 FIGURE 22.19 MRI of lymphoma. Axial T1-weighted fat-saturated MRI of the pelvis obtained after intravenous administration of gadolinium demonstrates multiple areas of diffuse enhancement in the bone marrow of the sacrum and pelvic bones and a soft-tissue mass (arrow). (Courtesy of Maria Teresa Guedez, MD, Maracay, Venezuela.) |
TABLE 22.1 Revised European American Lymphoma Classification | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
contended that in the early stages of myeloma, the pedicle (which does not contain as much red marrow as the vertebral body) is not involved, whereas even in an early stage of metastatic cancer the pedicle and vertebral body are both affected (Fig. 22.28). In the late stages of multiple myeloma, however, both the pedicle and vertebral body may be destroyed. Radionuclide bone scan can more reliably distinguish these two malignancies at this stage. It is invariably positive in cases of metastatic carcinoma, whereas in most cases of multiple myeloma, there is no increased uptake of radiopharmaceutical tracer. This phenomenon appears to reflect the purely lytic nature of most myelomatous lesions and the absence of significant reactive new bone formation in response to the tumor.
 FIGURE 22.20 Lymphoma in a child. Conventional radiograph of the right femur of a 7-year-old girl with groin pain and a fever reveals a destructive lesion of the diaphysis extending to the growth plate; there is also a lamellated type of periosteal reaction. Because of the age of the patient, the primary differential diagnosis included Ewing sarcoma, osteomyelitis, and Langerhans cell histiocytosis, all three of which may have a similar radiographic presentation in a long bone. The main factor differentiating these lesions is the duration of the patient’s symptoms. In this case, however, biopsy revealed a histiocytic lymphoma. |
 FIGURE 22.21 Lymphoma. Anteroposterior (A) and lateral (B) radiographs of the right knee of a 47-year-old woman, who had knee pain and initially was misdiagnosed with Paget disease, show a destructive lesion of the proximal tibia extending into the articular end of the bone. The mixed sclerotic and osteolytic character of this lesion may resemble the coarse trabecular pattern of Paget disease; however, there is a lack of cortical thickening. There is a pathologic fracture, but only a minimal periosteal response is evident. |
 FIGURE 22.22 Skeletal sites of predilection, peak age range, and male-to-female ratio in myeloma. |
 FIGURE 22.23 Variants in the radiographic presentation of myeloma. |
 FIGURE 22.24 Multiple myeloma. Involvement of the skull is prominent in this 60-year-old woman. Note the characteristic punched-out, lytic lesions, most of which are uniform in size and lack sclerotic borders. Occasionally, this pattern may be seen in metastatic disease. |
 FIGURE 22.25 Multiple myeloma. Lateral radiograph of the distal femur (A) and anteroposterior radiograph of the elbow (B) in a 65-year-old woman show endosteal scalloping of the cortex typical of diffuse myelomatosis. |
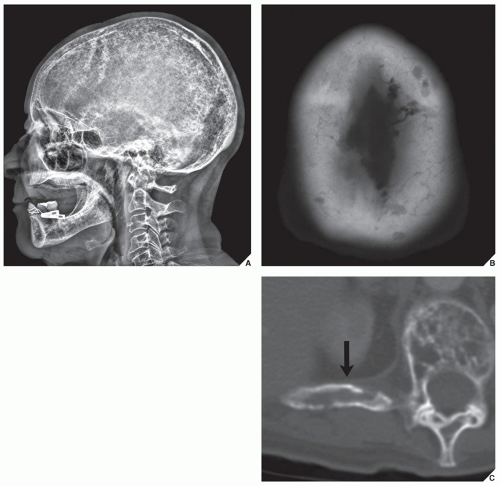 FIGURE 22.26 Multiple myeloma. (A) Lateral radiograph of the skull of a 76-year-old woman shows extensive involvement of the calvaria. Note also punched-out lesions in the mandible, not an unusual site of involvement. (B) CT image shows punched-out low-attenuated lesions in the occiput. (C) Axial CT section through the T10 vertebra shows involvement of the vertebral body and the adjacent right rib (arrow). |
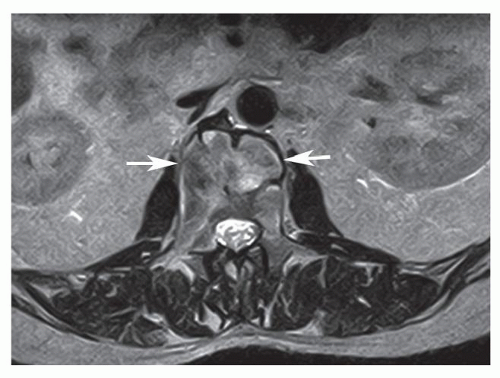 FIGURE 22.27 Multiple myeloma—mini brain sign. Axial T2-weighted MRI of the lumbar spine demonstrates expansion of the vertebral body (arrows) with anterior septa resembling the sulci of the brain. (Courtesy of Daniel Vanel, MD, Bologna, Italy.) |
Related posts:
 Radiologic Evaluation of Skeletal Anomalies
Radiologic Evaluation of Skeletal Anomalies
 Inflammatory Arthritides
Inflammatory Arthritides
 Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
Benign Tumors and Tumor-like Lesions II: Lesions of Cartilaginous Origin
 Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
Benign Tumors and Tumor-Like Lesions III: Fibrous, Fibroosseous, and Fibrohistiocytic Lesions
 Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
Benign Tumors and Tumor-Like Lesions IV: Miscellaneous Lesions
 Upper Limb III: Distal Forearm, Wrist, and Hand
Upper Limb III: Distal Forearm, Wrist, and Hand
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


