Fig. 2.1
Position of the patient during a brain study (a, b) and total body acquisition (c, d) (Discovery ST-E PET/CT system, General Electric Healthcare, Milwaukee, WI)
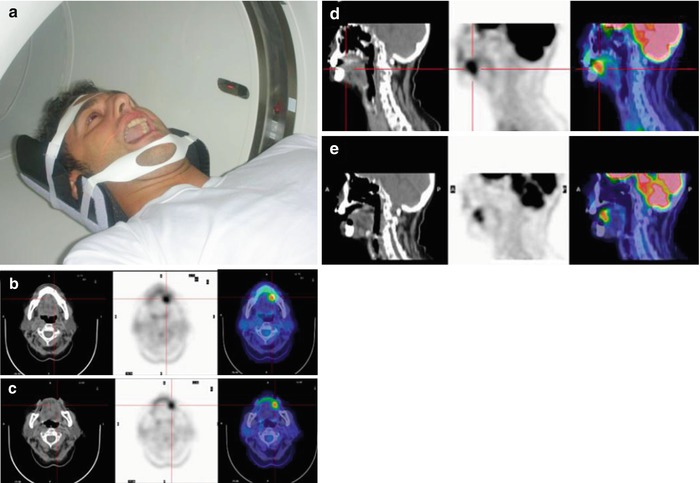
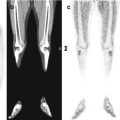
Fig. 2.2
(a) Open-mouth acquisition (Discovery ST-E PET/CT system, General Electric Healthcare, Milwaukee, WI). A 19-year-old male treated 10 years earlier for osteosarcoma of the tibia and now diagnosed with squamous carcinoma of the left border of the tongue. (b, c) Axial and sagittal projections of a conventional closed-mouth acquisition show pathological uptake in the left anterior mouth. Involvement of the mandibular bone or floor of the mouth is difficult to evaluate. (d, e) Axial and sagittal projections obtained in an open-mouth acquisition clearly show that the tumor is confined to the tongue
Since the patient must be in a fasting state beginning 4–6 h before the exam and for approximately 2 h during the exam and thereafter, the PET study should be scheduled early in the morning, shortly before breakfast, since, especially in children, a hungry patient is less likely to be compliant with the demands of the imaging study. A serum glucose level of 170 mg/dL in adults and 140 mg/dL in the pediatric patient is generally acceptable.
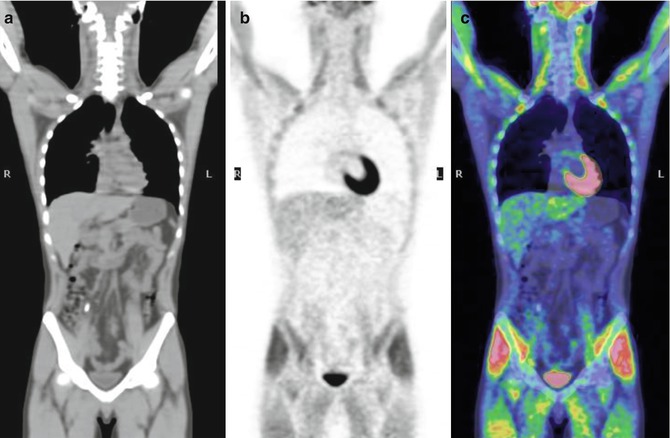
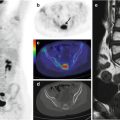
Fig. 2.3
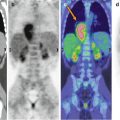
A 17-year-old male treated for Ewing’s sarcoma. The patient did not comply with the fasting requirement. Coronal CT (a), PET (b), and PET/CT (c) fusion images accordingly show diffuse 18F-FDG uptake by the skeletal muscles
In case of hyperglycemia, PET has a lower sensitivity in revealing disease because 18F-FDG competes with circulating glucose (Fig. 2.3) [1]. Thus, in children, once the typical diseases have been ruled out, if neoplasms involving the muscles (sarcomas) or other organs (e.g., hepatoblastoma) are suspected, an 18F-FDG–PET/CT study is warranted but with aggressive control of serum glucose levels in order to optimize the accuracy of the study. In diabetic patients, this can be achieved with fast-acting insulin. If a good glycemic level proves to be challenging, we recommend the protocol used in our center: 250 mL of saline solution (NaCl 0.9 %) containing 100 IU fast-acting insulin/L is infused at a maximum rate of 50 mL/h until the serum glucose is reduced to a correct level. Thirty minutes later, the radiotracer is injected. For nursing infants, the injection should be administered before the next milk feed [3] which should be 20–30 min later.
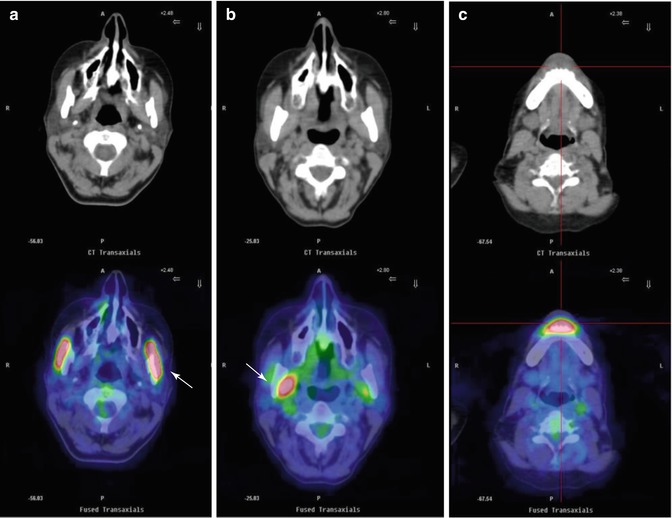
Both the child and his/her parents should be fully informed of the details of the imaging study, including the potential role of 18F-FDG–PET/CT in disease management and the absolute and relative (vs. a common exam such as X-ray or CT scan) radiation doses. Given the complexity of the procedure for the patient and family, it is important to ensure that they fully understand the procedure as this will greatly facilitate compliance. Similarly, it is essential to establish a good relationship with the child before and after tracer injection. This relationship should be tailored to the child’s developmental stage. A child who cries during the uptake phase will activate the diaphragm and intercostal muscles; continuous movement of the facial muscles, such as by chewing, during the uptake phase will activate the salivary glands and buccal cavity muscles (Fig. 2.4); in a child distracted by video games, the extraocular muscles and those of the upper limbs will be activated (Fig. 2.5). Also, the activation of brown adipose tissue, as will occur in a child who waits in a cold room during the uptake phase, must be avoided (Figs. 2.6 and 2.7). Brown adipose tissue is mostly present in the laterocervical regions of the neck, paravertebral thoracic regions, mediastinum, and epiphrenic area as well as around the kidneys and adrenal glands. Its activation can be mistakenly attributed to disease, leading to upstaging during the cancer staging phase and underestimation of the efficacy of therapy during treatment evaluation.