Cholecystocholedochal fistula: Contrast directly passes from biliary tree into GB
• MR: Dilated CHD and intrahepatic ducts with stricture at level of stone (signal void on all pulse sequences)
Site of CHD narrowing may appear thickened and hyperenhancing due to inflammation on T1WI C+
GB often thickened and inflamed due to concomitant cholecystitis
• US: Large, immobile gallstone impacted in cystic duct or infundibulum with dilated intrahepatic ducts
• CT: May be difficult to recognize stones
TOP DIFFERENTIAL DIAGNOSES
• Choledocholithiasis
• Cholangiocarcinoma, GB carcinoma, or regional lymphadenopathy
• Benign biliary stricture
PATHOLOGY
• Impaction of stone in cystic duct, infundibulum, or Hartmann pouch compressing bile duct at same level
Obstruction may be due to direct mass effect or development of stricture in CHD due to inflammation
• Predisposing factors: Long cystic duct running parallel to CHD or low insertion of cystic duct into common bile duct
• Cholecystocholedochal fistula may develop due to chronic inflammation/pressure necrosis, with gallstones eroding from cystic duct into bile duct
CLINICAL ISSUES
• Common symptoms: Fever, jaundice, RUQ pain (symptoms of obstructive jaundice, acute cholecystitis, cholangitis)
• Definitive treatment is surgical, with approach determined by type of Mirizzi syndrome
(Left) Graphic of Mirizzi syndrome depicts a large cystic duct stone causing extrinsic compression of the common hepatic duct (CHD) and dilation of the intrahepatic bile ducts .
(Right) Coronal T2WI MR shows subtle intrahepatic bile duct dilation and a large gallstone impacted within the neck of the gallbladder (GB), causing extrinsic narrowing of the common duct.
(Left) Coronal CECT shows a cystic duct stone that causes extrinsic compression of the CHD . The intrahepatic ducts were dilated, which was better seen on axial sections (not shown).
(Right) Coronal CECT demonstrates a large gallstone in the GB neck compressing the adjacent CHD , resulting in mild intrahepatic biliary dilatation (not shown). Note the dilated GB with multiple stones and mild wall thickening.
TERMINOLOGY
Definitions
• Partial or complete obstruction of common hepatic duct (CHD) due to gallstone impaction in cystic duct, infundibulum, or Hartmann pouch of gallbladder (GB)
IMAGING
General Features
• Best diagnostic clue
Impacted cystic duct stone causing extrinsic mass effect on CHD with resultant dilatation of intrahepatic ducts
• Morphology
Smooth extrinsic narrowing of CHD
Radiographic Findings
• ERCP
Extrinsic narrowing of CHD, dilated intrahepatic ducts, and lack of GB opacification
– Extrinsic impression on CHD is often concave to the right due to typical orientation of cystic duct relative to CHD
Probably best modality for identifying cholecystocholedochal fistula, with contrast seen to directly pass from dilated biliary tree into GB
Accuracy of ERCP for Mirizzi syndrome: 55-90%
MR Findings
• MRCP or T2WI can nicely demonstrate gallstones, with ≥ 1 stone impacted in GB neck or cystic duct
Gallstones usually appear as signal voids on all pulse sequences
Dilated CHD proximal to level of stone, discrete stricture or narrowing at level of stone, and more distal bile duct appearing decompressed
• Site of stricture or narrowing may appear thickened and hyperenhancing due to inflammation on T1WI C+
May be mistaken for tumor (such as cholangiocarcinoma)
• GB often thickened and inflamed due to concomitant cholecystitis
• MRCP can also demonstrate anatomic variants that might predispose to Mirizzi syndrome, including low insertion of cystic duct and long cystic duct running parallel to CHD
Ultrasonographic Findings
• Large, immobile gallstone impacted in cystic duct or infundibulum with dilated intrahepatic ducts proximal to level of stone
• Most patients have multiple other stones in GB
• Findings of cholecystitis frequent (GB wall thickening, wall hyperemia on color Doppler, pericholecystic fluid, positive sonographic Murphy sign)
GB may be contracted and thickened due to chronic cholecystitis
CT Findings
• Imaging findings similar to MR or US, with large stone in cystic duct, focal narrowing of CHD at level of stone, and biliary dilatation upstream from level of stone
More difficult to recognize stones on CT than on MR or US, and may be difficult in some cases to distinguish stone from soft tissue mass or tumor
If stone is recognized, multiplanar reformats are essential for properly identifying location of stone (within cystic duct rather than CHD) and appreciating mass effect of stone on adjacent common duct
• CT may be helpful for identifying other findings that may suggest tumor, including liver metastases, soft tissue mass in porta hepatis, etc.
Only gold members can continue reading. Log In or Register to continue




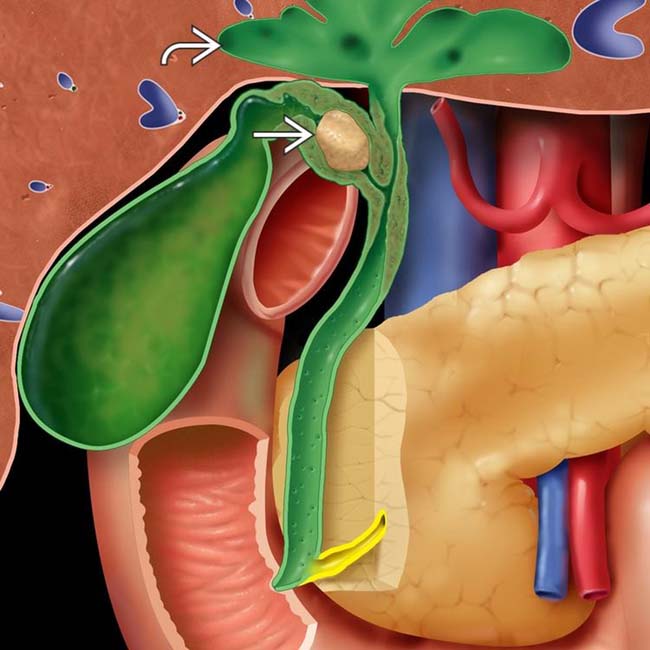
 causing extrinsic compression of the common hepatic duct (CHD) and dilation of the intrahepatic bile ducts
causing extrinsic compression of the common hepatic duct (CHD) and dilation of the intrahepatic bile ducts  .
.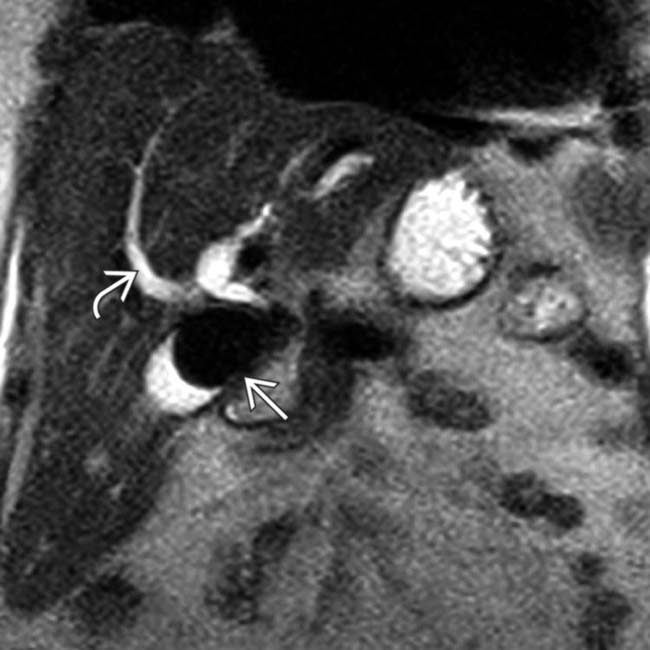
 and a large gallstone
and a large gallstone  impacted within the neck of the gallbladder (GB), causing extrinsic narrowing of the common duct.
impacted within the neck of the gallbladder (GB), causing extrinsic narrowing of the common duct.
 that causes extrinsic compression of the CHD
that causes extrinsic compression of the CHD  . The intrahepatic ducts were dilated, which was better seen on axial sections (not shown).
. The intrahepatic ducts were dilated, which was better seen on axial sections (not shown).
 in the GB neck compressing the adjacent CHD
in the GB neck compressing the adjacent CHD  , resulting in mild intrahepatic biliary dilatation (not shown). Note the dilated GB with multiple stones
, resulting in mild intrahepatic biliary dilatation (not shown). Note the dilated GB with multiple stones  and mild wall thickening.
and mild wall thickening.








 More difficult to recognize stones on CT than on MR or US, and may be difficult in some cases to distinguish stone from soft tissue mass or tumor
More difficult to recognize stones on CT than on MR or US, and may be difficult in some cases to distinguish stone from soft tissue mass or tumor




