and Filiz Özülker1
(1)
Nuclear Medicine, Okmeydani Training and Research Hospital, Istanbul, Turkey
18.1 Case 1: Carcinoma of Unknown Primary
History
A 54-year-old female underwent tru-cut biopsy from mass lesions detected on USG at liver and histopathology revealed metastasis of adenocarcinoma. A 18F-FDG PET/CT scan was performed to evaluate the extent of the disease and determine the primary site of malignancy.
Findings

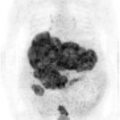
Fig. 18.1
MIP image shows intensely hypermetabolic mass lesions at both lobes of liver and a hypermetabolic lesion at sigmoid colon
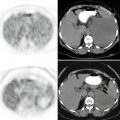
Fig. 18.2
Axial CT and PET images show multiple hypermetabolic mass lesions at both lobes of liver (a, b) and increased FDG uptake corresponding to the mass lesion at sigmoid colon (arrow) (c, d)
Interpretation
Hypermetabolic lesions at liver representing metastases from primary malignant lesion at sigmoid colon.
Teaching Point
Adenocarcinoma is the most commonly encountered histology among patients with CUP. Most patients have a small primary tumor that can metastasize, and the metastases grow while the primary tumor usually remains small.
18.2 Case 2: Incidentally Found Prostate Adenocarcinoma
History
A 71-year-old male who was being followed up with the diagnosis of lung cancer underwent 18F-FDG PET/CT for restaging.
Findings
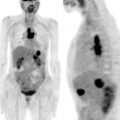
Fig. 18.3
MIP image shows intensely increased FDG uptake at right lung and a right supraclavicular lymph node (a). On axial PET, CT, and fusion images (b, d) there is incidentally found significantly hypermetabolic focus at prostate gland (arrow)
Interpretation
Hypermetabolic lesions at right lung are compatible with primary lung cancer and there is also a metastatically involved right supraclavicular lymph node. Focal hypermetabolic lesion at prostate gland is suspicious for malignancy.
Result
Biopsy from the lesion at prostate gland revealed adenocarcinoma.
Teaching Point
Although prostate adenocarcinomas show generally no or mild FDG uptake, poorly differentiated cancers or those with a rapid cell turnover may exhibit increased FDG uptake and show FDG-avid areas within the prostate. Since the benign lesions can also show FDG uptake, it is not always easy to decide whether a hypermetabolic lesion at prostate gland is benign or not.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


