12 | Multiple Pregnancy and Doppler Ultrasound |
Multiple pregnancies are one of the indications for Doppler ultrasound in obstetrics that are included in many guidelines, especially when there is discordant growth of the infants.
Simple monitoring methods used successfully for single fetuses, such as inspection, palpation, fundal height, abdominal girth, etc., fail to provide information about an individual infant in a multiple pregnancy. For this reason ultrasound techniques such as cardioto-cogram (CTG), ultrasound, Doppler ultrasound, and color Doppler ultrasound are indispensable aids when multiple pregnancies are being monitored.
The more closely the multiple fetuses are linked, the more important becomes the use of biophysical methods. In the case of dichorionic multiple fetuses (Fig. 12.1) constrictions in nutritional supply are the primary problem because they may result in discordant or restricted growth. In monochorionic multiple pregnancies additional problems arise with communications between the fetal circulations such as a twin-to-twin transfusion syndrome (TTTS), (feto–fetal transfusion syndrome [FFTS]) or twin reversed arterial perfusion (TRAP). Finally, in monoamniotic twins (Fig. 12.2) complications play an important role. This chapter will only briefly refer to the special morphological and functional problems of conjoined twins.
Doppler ultrasound is part of the risk assessment in the second half of pregnancy. Discordant growth is a specific indication during this time, beside the indications arising during singleton pregnancies. In the author’s opinion every twin pregnancy, but especially every monochorionic twin pregnancy, should in itself be an indication for Doppler ultrasound examination. The reasons for this will be clear by the end of this chapter.

Fig. 12.1 Display of a dichorionic twin pregnancy.
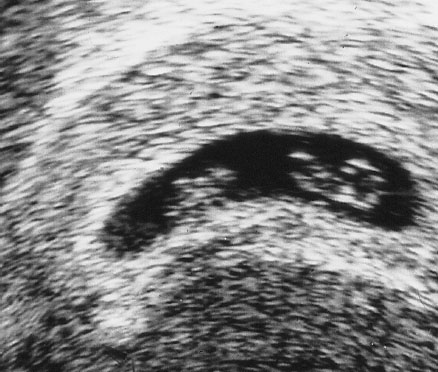
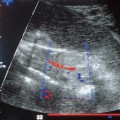
Fig. 12.2 Display of a monoamniotic twin pregnancy.
Studies Using Doppler Ultrasound for Multiple Pregnancies
Monitoring multiple pregnancies by Doppler ultrasound was considered promising from a relatively early stage. Selective display of hemodynamic parameters was especially well accepted, since, as mentioned earlier, the simpler methods for assessing risk in single pregnancies are often ineffective in multiple pregnancies.
Consequently, some studies were undertaken as early as the 1980s using Doppler ultrasound examinations for screening, but also to evaluate previously established risks. However, diagnostic studies of the fetal membranes to determine chorionicity for the assessment of risk, which have been especially valuable lately, were not yet as developed when those studies appeared.
In 1985 Giles et al. published the first larger study of the use of Doppler ultrasound in 76 multiple pregnancies. They examined the S/D ratio (the ratio between the systolic maximum [S] and the diastolic minimum [D] of the waveform) in the umbilical aa.. Abnormal elevation of the S/D ratio identified growth-restricted fetuses in 26 out of 33 cases, while normal values were found in all 32 pregnancies in which the infants were of normal size. The sensitivity was 0.79; the specificity 1. By contrast, the early results from studies linking discordant growth with presumed TTTS were rather anecdotal in nature.
Giles et al. (1993) investigated whether factors interfering with growth were preplacental or placental. They were able to show that when Doppler findings in a twin were abnormal and growth was restricted this was accompanied by selective placental pathology. In these cases they did not see this as a sign of preplacental pathology, as might be assumed in single pregnancies with growth restriction and abnormal Doppler findings in the maternal uterine aa.
In 1987 Nimrod et al. published a study designed to find indicators for an unfavorable course for a pregnancy. They determined the S/D ratio in the umbilical aa. and the descending aorta together with the pulsatility index (PI). They also determined flow volumes in the aorta. In summary, their results showed that some individual readings as well as the indices, especially flow volume, were of almost identical value in predicting an unfavorable outcome of the pregnancy. The sensitivity was 0.50; the specificity 0.89. Doppler ultrasound was considered to be a very promising addition to the armamentarium.
Gerson et al. (1987) conducted a Doppler study on 52 twin pregnancies and four sets of triplets designed to diagnose discordant growth in twins as early as possible. The result was a fairly good predictive value, which was not possible by other methods. The sensitivity was 0.82; the specificity 0.98, with a high kappa of 0.82.
Saldana and co-workers (1987) chose a rather complex approach. They tried to register differences in the S/D ratio >0.4 in 69 twin pregnancies and to find differences in weight of >350 g in the third trimester between the pairs of twins. The outcome was disappointing, resulting in a predictive value of 0.42. On the other hand, the predictive value for a normal weight when the S/D ratio was <0.4 was much more favorable at 0.91.
The first such study was attempted by Farmakides et al. (1985), who investigated 43 twin pregnancies. They, however, calculated a sensitivity of 0.73 and a specificity of 0.82. The question that arises for both studies is whether the selected approach, namely looking for differences by pairs, is practical.
The influence on clinical management and perinatal data of Doppler ultrasound examination of the umbilical aa. between the 28th and 32nd weeks of gestation was addressed by Trudinger’s group (1988). Revealing the results of the Doppler examination to the attending physicians in the test group, while for a control group Doppler data were simply collected under blind conditions, showed a distinct reduction in perinatal mortality, fetal deaths, and utilization of neonatal intensive care.
In 1990 the same working group found a similarly convincing result in triplet pregnancies, with a close link between changes in the Doppler sonogram of the umbilical aa. and developmental delays in individual triplets.
Hastie et al. in 1989 found the results of Doppler ultrasound less convincing. They examined the umbilical aa. in 89 twin pregnancies at monthly intervals and found a sensitivity of 0.29 at a predictive value of 0.34 for growth restriction.
Divon et al. in 1989 examined 58 twin pregnancies in the third trimester. They found that the 18 discordant fetuses could not be detected in all cases with any of the methods they used, including Doppler sonography of the umbilical aa. A positive predictive value of 0.73 and a negative predictive value of 0.90 were only achieved by a combination of biological measurements and Doppler ultrasound.
In 1991 Gaziano et al. arrived at the conclusion that Doppler ultrasound can make a valuable contribution to the monitoring of multiple pregnancies when they examined pregnancies involving 94 pairs of twins and seven sets of triplets.
Related posts:
 Diagnosis of the Uterine Tube by Transvaginal Sonography
Diagnosis of the Uterine Tube by Transvaginal Sonography
 Doppler Sonography in Obstetrics—Screening At-Risk Populations
Doppler Sonography in Obstetrics—Screening At-Risk Populations
 Doppler Ultrasound Findings Near Term
Doppler Ultrasound Findings Near Term
 Doppler Ultrasound in the Diagnosis of Fetal Anomalies
Doppler Ultrasound in the Diagnosis of Fetal Anomalies
 Diagnostic Sonography of Blood Flow in Breast Tumors
Diagnostic Sonography of Blood Flow in Breast Tumors
 Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


