Case presentation
A 6-year-old female presents with persistent, worsening right knee swelling for the past 2 months. The area has become painful over the past few weeks, especially at night. There has been no fever, erythema, or swelling of the other extremities or joints. There is no report of trauma, but prior to the development of symptoms, the child was quite physically active and it is possible that she may have injured the knee while playing. The child’s physical examination is remarkable for generalized swelling of the right knee. She has minimal pain to palpation of the superior aspect of the knee; full extension of the knee produces pain. There is no warmth, erythema, or fluctuance.
Imaging considerations
Plain radiography
A two-view radiographic examination of the involved extremity is reasonable first-line imaging in pediatric patients with extremity complaints and is often utilized in trauma settings. Clinical prediction rules have been developed to assist the clinician in identifying which trauma patients may benefit from imaging. In selected patients, such as those who have sustained trauma, additional views may be needed. For example, a sunrise view can be used to assess the patella for fracture or subluxation, which may not be visualized on a two-view study.
Children with knee pain, especially chronic pain, who have no signs of abnormality on their clinical examination typically will have imaging of the involved knee. However, the possibility of referred pain should be considered. A common scenario illustrating this is referred pain from the hip with a slipped capital femoral epiphysis or Legg-Calve-Perthes disease. In these cases, imaging of the hip (anterior-posterior [AP] and frog leg views) is appropriate while also imaging the involved knee.
Computed tomography (CT)
Non–contrast-enhanced CT is generally not a first-line imaging study in pediatric knee complaints. It may be employed to better visualize fractures such as patellar or tibial plateau fractures and to evaluate joint involvement if a fracture is present. In children with identifiable bone masses, CT is used to look for metastatic lesions, especially in the thorax.
Magnetic resonance imaging (MRI)
While generally not a first-line imaging modality, MRI is a more definitive study to visualize joint spaces, ligaments, and tendons and evaluate tumoral, inflammatory, or infectious processes. MRI is used to further evaluate masses that are initially detected through other modalities.
Imaging findings
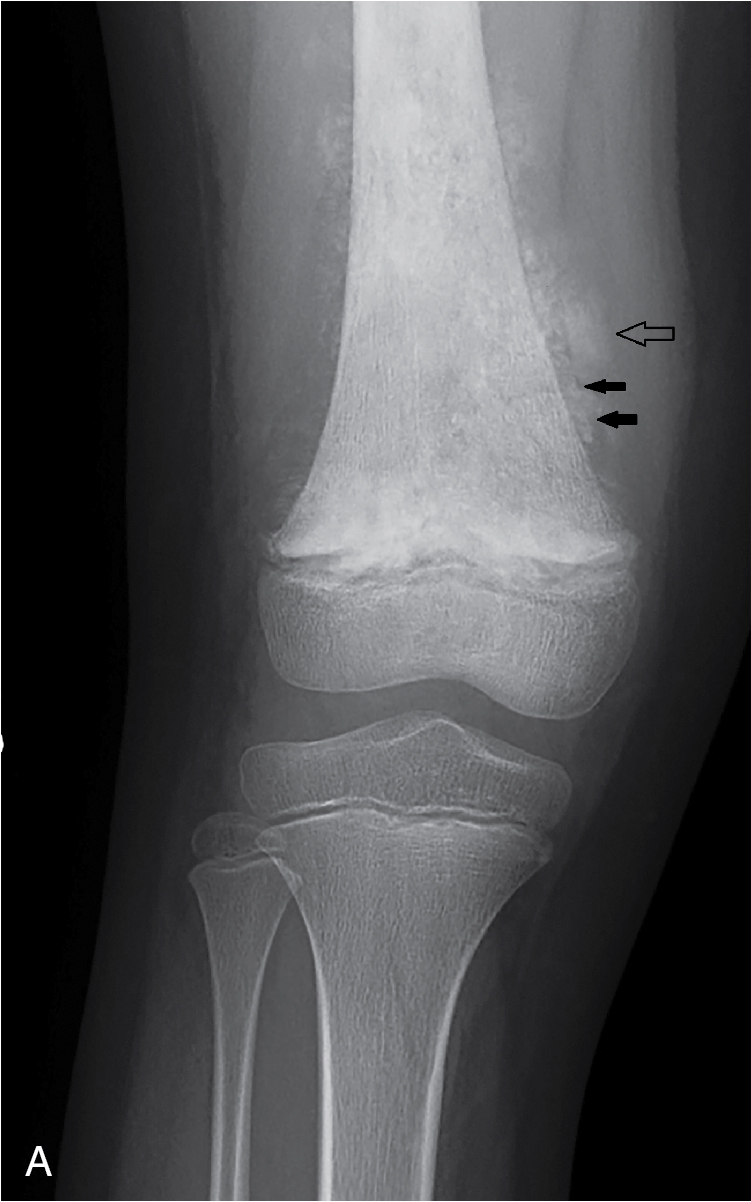
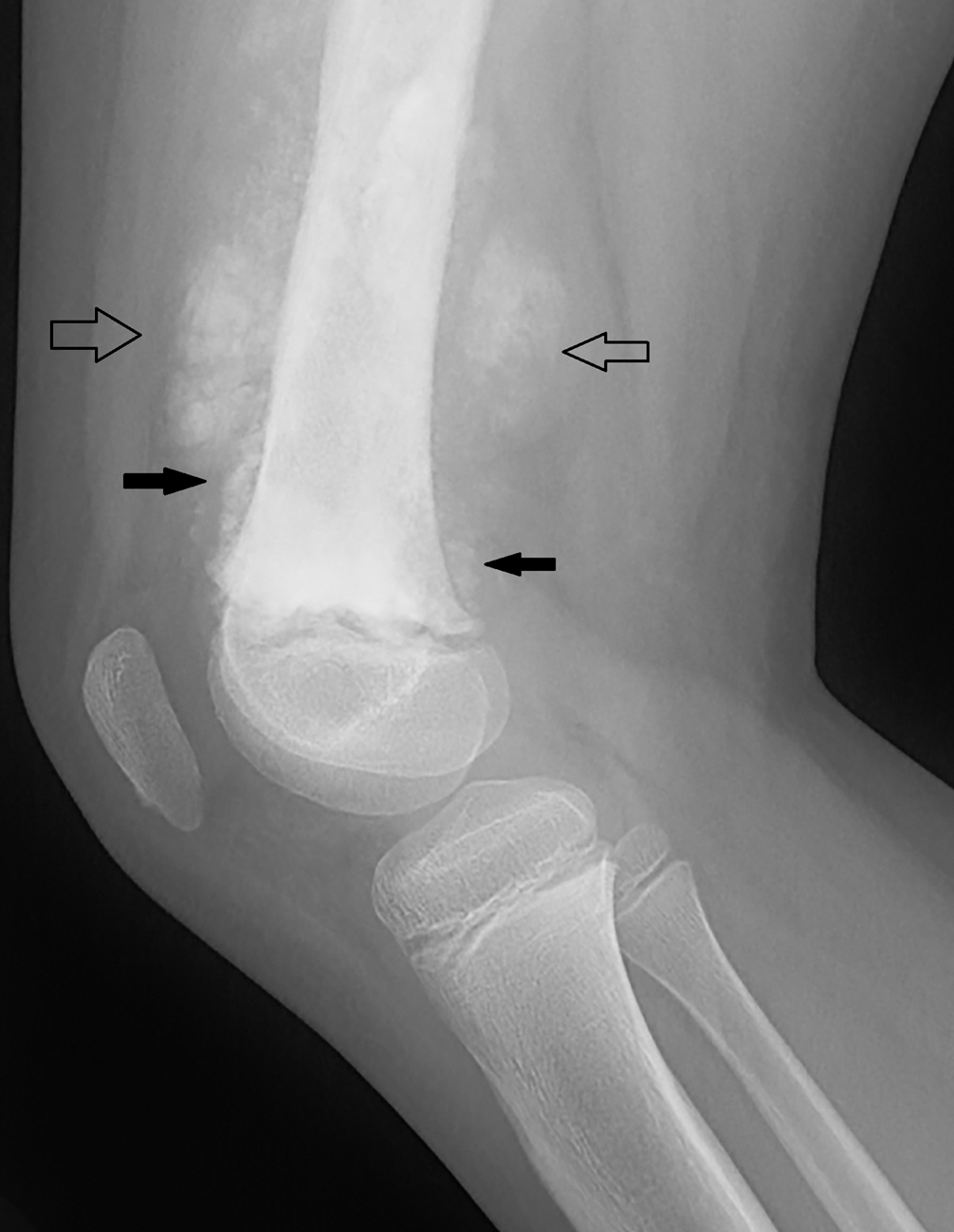
The child had three views performed of the right knee. These images reveal abnormal sclerosis of the distal femoral diaphysis and metaphysis, discontinuous periosteal new bone, and cloudlike calcification around the distal femur, with extension into the surrounding soft tissues ( Figs. 78.1A–78.3 ). Because of the possibility of trauma, a sunrise view was also obtained; there is no fracture ( Fig. 78.4 ). The findings noted on plain radiography suggest an aggressive process, with the ossification extending into the soft tissues most suggestive of osteosarcoma.