TABLE 21.1 Per-Vessel Diagnostic Performance of Multidetector CT in Prediction of Hemodynamically Significant Stenoses Compared with Invasive Fractional Flow Reserve | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 21.2 Per Vessel Diagnostic Accuracy of Noninvasive Stress Imaging Compared with Invasive Fractional Flow Reserve | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 21-1. The “one-stop” anatomical and functional coronary assessment using cardiac CT. |
 Figure 21-2. Perfusion defects (arrows) demonstrated using a canine model of LAD ischemia. (Adapted from George RT, Silva C, Cordeiro MA, et al. Multidetector computed tomography myocardial perfusion imaging during adenosine stress. J Am Coll Cardiol 2006;48:153-160, with permission from Elsevier.) |
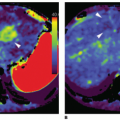
 Figure 21-3. Dynamic and static CTP. This graph shows typical time-attenuation curve (TAC) acquired by dynamic CT MPI and two static images of the same midventricular slice, corresponding to different time points of CT MPI scan. The orange curve (I) in the graph represents the TAC in normal tissue, the purple curve (II) that of ischemic myocardium. The green curve (III) is the TAC of the ascending aorta. Differences in enhancement between normal and ischemic myocardium are maximal during upslope of myocardial bolus passage. Image (A) was taken at the time point indicated by line A in the graph during contrast upslope. Image (B) was taken 6 s later as indicated by line B during early contrast downslope. The variation between the images emphasizes that timing of CT image acquisition is paramount for MPI assessment. (Adapted from Ho KT, Chua KC, Klotz E, et al. Stress and rest dynamic myocardial perfusion imaging by evaluation of complete time-attenuation curves with dual-source CT. JACC Cardiovasc Imaging 2010;3:811-820, with permission from Elsevier.) |
 Figure 21-4. Advances in CT scanner technology. The advances, which have been most advantageous for perfusion imaging, include improvements in temporal resolution, increased longitudinal coverage, and decreased scan time. |
be completed after multiple gantry rotations over three to four heartbeats. Myocardial contrast attenuation hence varies between the superior and inferior aspects of the heart due to the lack of temporal uniformity when image acquisition spans multiple cardiac cycles.
TABLE 21.3 CT Scanners Used in Myocardial Perfusion Imaging—Strengths and Limitations | |||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||
within an ultrafast scan time of 0.25 to 0.27 seconds during one end-diastolic phase due to the fast table movement, which will also ensure temporal contrast enhancement throughout the entire myocardium.45
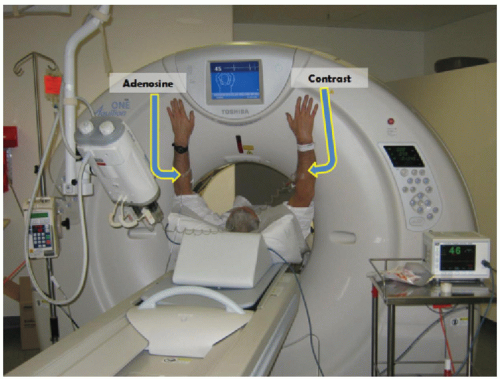 Figure 21-5. Image acquisition during coronary CT angiography/CT stress myocardial perfusion imaging (CCTA/CTP). Intravenous access is obtained in both antecubital veins for the administration of adenosine and iodinated contrast. The average time taken for the combined rest CCTA + stress CTP protocol on the CT table is 43 min. (From Ko BS, Cameron JD, Leung M, et al. Combined CT coronary angiography and stress myocardial perfusion imaging for hemodynamically significant stenoses in patients with suspected coronary artery disease: a comparison with fractional flow reserve. JACC Cardiovasc Imaging 2012;5:1097-1111.) |
stress scans, respectively, were performed as the second scan. The advantage of the stress followed by rest protocol is that the ability for the stress scan to detect ischemia is optimized. It will also allow the administration of nitrates for the subsequent rest scan, which may have otherwise been contraindicated if the rest scan was performed up front. On the contrary, initial rest-phase imaging more closely resembles clinical practice, where patients will only proceed to have CTP performed if a coronary stenosis of at least moderate severity is identified on resting CCTA. In our institution, we most often use a rest/stress sequence (Fig. 21-6).95 Contrast contamination can be avoided in our experience by leaving an interval of at least 20 minutes between the two scans to allow wash-out of contrast from the myocardium.17,50
TABLE 21.4 CCTA/CTP imaging sequence | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
 Figure 21-6. CCTA/CTP imaging protocol using 320-detector CT. (Adapted from Ko BS, Cameron JD, Defrance T, et al. CT stress myocardial perfusion imaging using multidetector CT—A review. J Cardiovasc Comput Tomogr 2011;5:345-356, with permission from Elsevier.) |
 Figure 21-7. Stepwise interpretation algorithm for CT-based anatomic/functional assessment. This starts with evaluation of the coronary CCTA (Step 1) followed by myocardial CTP image reconstruction (Step 2) and evaluation of CTP image quality (Step 3). Serial rest and stress images are then analyzed and compared for perfusion defects and other abnormalities associated with ischemia and infarction (Step 4). Finally, these analyses are correlated with anatomic localization of coronary stenoses on CCTA (Step 5). (Adapted from Mehra VC, Valdiviezo C, Arbab-Zadeh A, et al. A stepwise approach to the visual interpretation of CT-based myocardial perfusion. J Cardiovasc Comput Tomogr 2011;5:357-369, with permission from Elsevier.) |
 Figure 21-8. CCTA interpretation followed by CT perfusion assessment. The paradigm of CT-based cardiac risk assessment involves the use of CT angiography followed by CT perfusion if significant atherosclerosis is seen. As shown here, a moderate proximal LAD stenosis (A) is associated with an anterior and apical wall perfusion abnormality (arrows) just distal to the stenosis seen on stress myocardial CTP (C). These perfusion defects are reversible because they are absent on rest myocardial CTP (B). (Adapted from Mehra VC, Valdiviezo C, Arbab-Zadeh A, et al. A stepwise approach to the visual interpretation of CT-based myocardial perfusion. J Cardiovasc Comput Tomogr 2011;5:357-369, with permission.) |
 Figure 21-9. Example of images acquired during excessive cardiac motion. Cardiac motion during image acquisition can lead to ghosting of endocardial and epicardial edges and streaking (arrows). Presence of these features can make detection of perfusion abnormalities difficult and should mandate a search for alternative phases without motion. (Adapted from Mehra VC, Valdiviezo C, Arbab-Zadeh A, et al. A stepwise approach to the visual interpretation of CT-based myocardial perfusion. J Cardiovasc Comput Tomogr 2011;5:357-369, with permission.) |
 Figure 21-10. False-positive perfusion defect due to motion artifact in a patient who underwent adenosine perfusion scanning with a heart rate of 90 bpm. A: CT perfusion imaging showed apparent perfusion defects in the anterolateral and inferior walls (black arrows). B: Invasive coronary angiography (ICA) image of the LAD artery and large diagonal branch (which supplied the anterolateral wall) demonstrated no hemodynamically significant stenoses (fractional flow reserve [FFR] 0.92 in diagonal branch). C: ICA image of the right coronary artery also revealed no significant stenosis to account for apparent inferior ischemia. (Adapted from Nasis A, Seneviratne S, DeFrance T. Advances in contrast-enhanced cardiovascular CT for the evaluation of myocardial perfusion. Curr Cardiovasc Imaging Rep 2010;3:372-381, with permission.) |
 Figure 21-11. Beam-hardening artifact correction algorithm. Beamhardening artifacts appear as areas of hypoattenuation most commonly in the basal inferior wall (arrow). A: This wall is particularly vulnerable to this artifact because of its location being between the contrast-rich left ventricular cavity and descending aorta. B: Reconstruction kernels that implement beam-hardening correction algorithm are effective in overcoming this artifact (arrow). (Adapted from Mehra VC, Valdiviezo C, Arbab-Zadeh A, et al. A stepwise approach to the visual interpretation of CT-based myocardial perfusion. J Cardiovasc Comput Tomogr 2011;5:357-369, with permission.) |
Related posts:
 Vascular Anatomy and Microanatomy
Vascular Anatomy and Microanatomy
 CT and MR Contrast-Enhanced Tissue Perfusion Imaging: Basic Methodology, Postprocessing, Reliability Testing
CT and MR Contrast-Enhanced Tissue Perfusion Imaging: Basic Methodology, Postprocessing, Reliability Testing
 Clinical Applications of ASL Brain Perfusion Imaging
Clinical Applications of ASL Brain Perfusion Imaging
 Perfusion CT Imaging in Oncology
Perfusion CT Imaging in Oncology
 Ultrasound Perfusion Imaging: Techniques and Analytical Methods
Ultrasound Perfusion Imaging: Techniques and Analytical Methods
 Contrast-Enhanced Ultrasound: Clinical Applications
Contrast-Enhanced Ultrasound: Clinical Applications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


