the radiotracers that are used, it requires the presence of cyclotron within short distance from the laboratory for studies based on short-lived isotopes (see below).2
TABLE 23.1 Common Radiopharmaceuticals for Myocardial Perfusion Scan | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
and therefore, the radiopharmaceutical may be given in the second to third minute of the test, and the test may be finished over 2.5 to 3 minutes later. Like dipyridamole, adenosine can be coupled with submaximal dynamic exercise when tolerated to reduce the frequency and severity of adverse effects associated with vasodilator infusion.14 A bicycle ergometer, allowing a semirecumbent patient’s position, may be preferable to a treadmill, because intravenous infusions are easily managed when the patient is relatively steady. Heart rate, blood pressure, and ECG should be measured and recorded at baseline and every 2 minutes during the infusion. The tracer is injected between the 3rd and 4th minutes of the adenosine infusion or sooner if symptoms or other complications require.
TABLE 23.2 Stress Test Protocols | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
the myocardium, which depends on the type of tissue (soft tissue, bone, or lungs), the activity of the radiopharmaceutical, and the body type of the patient. The most common artifact is the appearance of an inferior defect in men due to attenuation of photons by the diaphragm or an anterior wall defect in women due to photon attenuation from the breast tissue7 (Table 23.3).
TABLE 23.3 Possible Causes of “Artifacts” during Imaging | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
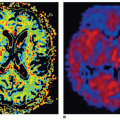
 Figure 23-1. Normal myocardial perfusion scintigraphy (MPS). Homogeneous radiotracer uptake in the walls of the left ventricle are shown. A: Apical (left) and basal (right) short axis slices. B: Horizontal long axis. C: Vertical long axis. D: Polar mapping of the same patient demonstrating normal myocardial perfusion. |
increased incidence of future cardiac events in patients with CAD. Lung uptake is a marker of impaired left ventricular function at rest or induced by ischemia during exercise. It is expressed as a ratio between uptake in the lungs and the myocardium, even though myocardial uptake depends upon viability and perfusion. The measurements are obtained either from an initial anterior planar image or from the appropriate image of the tomographic acquisition, and a normal lung:heart ratio is less than 0.55 ± 0.11.42 In a mechanism similar to that of 201Tl, the increased uptake of MIBI or tetrofosmin by the lungs and an LHR more than 0.35 ± 0.08 is associated with LV dysfunction and is a predictor of adverse prognosis in patients with known or suspected CAD.43,44 Perfusion defects are not always the result of CAD (see below). Abnormalities can be seen with coronary spasm, anomalous arteries, muscle bridges, small vessel disease as may occur in diabetes or syndrome X, the dilated and hypertrophic cardiomyopathies, hypertrophy caused by outflow obstruction or hypertension, infiltrative disorders such as sarcoidosis and amyloidosis, connective tissue disorders, and conduction defects such as LBBB.
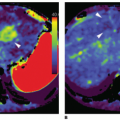
 Figure 23-2. Reversible perfusion abnormality in the anteroapical region and the septum superimposed upon minor partial thickness damage at the apex. The perfusion defect is more pronounced towards the apex. The overall appearances are compatible with left anterior descending (LAD) disease. A: Long axis. B: Short axis. C: Polar maps. |
a short course is divided into the anterior descending artery (LAD) and the circumflex artery (LCX). The LAD feeds the anterior wall and the upper 2/3 of the septum, while the LCX feeds the lateral LV wall and sometimes also the base of the inferior wall. In 85% of cases, the right is the dominant (right dominance), giving rise to the posterior descending artery (PDA). In the rest of the cases, PDA stems from the circumflex artery (left dominance) and perfuses the inferior wall and the lower part of the intraventricular septum or (rarely) from both the LCX and the RCA (codominance).48 Exact matching of anatomical damage and ischemia may be achieved by hybrid imaging, combining CT coronary angiography with SPECT MPI49,50
 Figure 23-3. Image interpretation: Assessment of extent and severity of perfusion defects. Short-axis views of four different patients are presented demonstrating a range of perfusion abnormalities (from mild and limited at the left upper corner to extensive and severe at the right lower corner). The extent of a perfusion abnormality is defined by the number of abnormal segments involved, while the severity is determined by the reduction of uptake in each segment. Tracer uptake within a segment is classified as normal; mildly, moderately, or severely reduced; or absent. These categories reflect the counts as a percentage of maximum in the whole set of tomograms. For each category, a score is given, so that SSS, SRS, and SDS can be calculated. Based on the SSS, perfusion images can be classified as normal (SSS 0-3), mildly abnormal (SSS 4-8), or moderate-severely abnormal (SSS ≥ 9). |
 Figure 23-4. Seventeen-segment model as per American College of Cardiology/American Heart Association (ACC/AHA) recommendations. The left ventricle (LV) has four walls (anterior, septum, inferior, and lateral) and an apex. The LV myocardium can be divided into a certain number of segments, for example, 9, 12, 14, 17 (as it is shown here and recommended by the ACC/AHA), or twenty. |
 Figure 23-5. Examples of myocardial ischemia (A) of the inferior wall and (B) the lateral wall. |
are similar while the phase histogram of the ventricles consists of a small amplitude peak. In cases of myocardial ischemia, fibrosis, or conduction disorders, there is enlargement of the histogram.25 The imaging parameters most helpful for predicting response to CRT are histogram bandwidth and phase SD (Fig. 23-7).
 Figure 23-6. Myocardial perfusion scintigraphy (MPS) with ECG-gated SPECT. End-diastolic and end-systolic images, representative images of polar mapping, and 3D images of regional wall motion (A). Normal EF and normal end-diastolic and end-systolic volumes (B). |
 Figure 23-7. A: Example of a patient without LV dyssynchrony on ECG-gated SPECT MPI. Synchronous contraction pattern is reflected by homogeneous phase angle distribution of polar map (left) and narrow highly peaked histogram (right). B: Example of a patient with extensive LV dyssynchrony on ECGgated SPECT MPI. LV dyssynchrony is indicated by heterogeneous phase angle distribution of polar map (left) and wide histogram (right). (Reprinted by permission of the Society of Nuclear Medicine, Boogers MM, Van Kriekinge SD, Henneman MM, et al. Quantitative gated SPECT-derived phase analysis on gated myocardial perfusion SPECT defects left ventricular dyssynchrony and predicts response to cardiac resynchronization therapy. J Nucl Med 2009;50:718-725.) |
it is based on sympathetic stimulation. Release of norepinephrine from stimulated sympathetic neurons activates α-adrenoceptors on the endothelium that mediate the release of nitric oxide. In the presence of an intact endothelium, this leads to a 30% to 65% increase in myocardial blood flow (MBF) compared to baseline levels. α-Adrenergic stimulation of vascular smooth muscle cells that causes vasoconstriction is normally counteracted; however, if endothelial integrity is impaired, it prevails over the endothelium-derived vasodilatation. CPT is probably the most appropriate test for early detection of endothelial dysfunction in individuals with risk factors for coronary atherosclerosis, as impairment of the endothelial health precedes abnormalities in smooth muscle cell vasodilator function, but requires extensive procedural standardization.2,51,53
 Figure 23-8. Qualitative assessment of myocardial perfusion by stress/rest 13N-ammonia PET. Stress and rest images from a 69-year-old man demonstrating a small area of myocardial infarction at the basal inferior wall and also extensive inducible ischemia involving most of the remaining viable myocardium sparing only the basal septum and the adjacent basal part of the anterior wall. PET, positron emission tomography. |
comorbidities such as severe peripheral vascular disease or diabetes, and uncontrolled CAD risk factors, contribute to the annual risk of cardiac events, which may be classified as low (<1%), intermediate (1% to 3%), or high (>3%).63 Numerous studies have confirmed the excellent prognostic power of SPECT MPI and its important role in risk stratification and patients’ management.64,65 and 66 In addition, SPECT MPI provides incremental information over and above that obtained by clinical or stress ECG data. Several large studies reporting prognostic analyses of MPI in cohorts using exercise, vasodilator, or both types of stress in various clinical settings have documented the incremental value of MPI.67,68 and 69 The incremental value of SPECT MPI can be increased further for assessing the probability of death due to cardiovascular causes by incorporating information on LVEF and LV end-systolic volume derived from the gated data.
TABLE 23.4 High-Risk Imaging Variables | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:
 Vascular Anatomy and Microanatomy
Vascular Anatomy and Microanatomy
 CT and MR Contrast-Enhanced Tissue Perfusion Imaging: Basic Methodology, Postprocessing, Reliability Testing
CT and MR Contrast-Enhanced Tissue Perfusion Imaging: Basic Methodology, Postprocessing, Reliability Testing
 Clinical Applications of ASL Brain Perfusion Imaging
Clinical Applications of ASL Brain Perfusion Imaging
 Perfusion CT Imaging in Oncology
Perfusion CT Imaging in Oncology
 Ultrasound Perfusion Imaging: Techniques and Analytical Methods
Ultrasound Perfusion Imaging: Techniques and Analytical Methods
 Contrast-Enhanced Ultrasound: Clinical Applications
Contrast-Enhanced Ultrasound: Clinical Applications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


