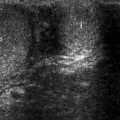
Fig. 9.1
Squamous cell carcinoma of the penis infiltrating the corpora cavernosa in an 81-year-old patient. Longitudinal ultrasound scan shows the tumor (*) causing interruption (curved arrows) of the echogenic line of the tunica albuginea (arrowheads) at the tip of the corpora cavernosa
In patients with initial infiltration, ultrasonography may show a thickened tunica albuginea in contact with the tumor which is not interrupted, but is less echogenic than in the remaining portions. Local staging of large tumors extending to the pelvis cannot be obtained with ultrasound. Evaluation of these lesions requires other imaging modalities, in particular, magnetic resonance imaging.
Computed Tomography
In advanced penile cancers, CT has a role in identification of distant metastatic deposits. It is also indicated in patients with lymphoma to check for presence of other localizations of the disease.
The sensitivity of CT in assessment of pathological nodes, however, is limited.
CT suffers from the inability to detect metastasis in normal-sized nodes, as lymph node enlargement may be caused by inflammation.
Magnetic Resonance Imaging
MR imaging is the gold standard modality for staging primary penile malignancies. Compared with ultrasound, this technique provides better contrast resolution, the margins between the mass and the erectile bodies are more clearly visualized, and better tumor staging is obtained.
Different imaging protocols can be used. In general, when the tumor is small, superficial coils are preferred to obtain a better spatial resolution. In patients with large tumors, the pelvic coil is used to produce images of the entire pelvis along different planes and obtain information on invasion of adjacent organs.
At least an axial T1-weighted and axial, sagittal, and coronal T2-weighted sequences should be produced. If gadolinium is administered, fat-saturated T1-weighted images should be obtained on the three planes before and after contrast administration. Axial T1-weighted images of the pelvis are obtained using a pelvic coil to look for inguinal and obturator lymphadenopathy. As occurs for ultrasound, intracavernosal PGE1 injection is recommended.
In general, this tumor is hypointense or isointense relative to the corpora on T1-weighted images and hypointense on T2-weighted images (Fig. 9.2a).
Fig. 9.2
A 58-year-old patient with penile cancer. (a) Sagittal T2-weighted MR image demonstrates tumor infiltration of the tip of the left corpus cavernosum (*) presenting as a hypointense area. (b) Tumor infiltration (*) appears with poor contrast enhancement on gadolinium-enhanced T1-weighted image
Compared with the corpora, poor enhancement is usually observed (Fig. 9.2b).
T2-weighted and gadolinium-enhanced T1-weighted images are the most useful sequences in defining the local extent of the disease. The depth of tumor invasion and involvement of the tunica albuginea, corpora, or urethra can be determined.
A recent study on a series of 55 tumors shows a sensitivity of 89, 75, and 88 % and a specificity of 83, 89, and 98 % in staging correctly tumors confined to subepithelial connective tissue, infiltrating the corpora and invading the urethra and prostate.
Pathology
Patients with penile squamous cell carcinoma range in age from 20 to 90 years, with an average of about 60 years. They present with an exophytic mass, an ulcer, or an area of mucosal erythema (Fig. 9.3).
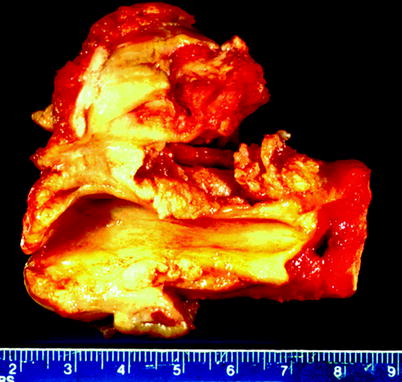
Fig. 9.3
Squamous cell carcinoma. Distal penectomy specimen showing invasive squamous cell carcinoma, involving glans penis, corpus spongiosum, and corpora cavernosa
Almost all penile squamous cell carcinomas originate in the mucosal epithelium of the glans (most common), coronal sulcus, or foreskin. Primary carcinoma of the skin covering the shaft and foreskin is rare.
Microscopically, squamous cell carcinoma is composed of malignant squamous cells forming fungating exophytic masses or ulcerative lesions infiltrating the underlying structures (Fig. 9.4). Tumors are graded according to the degree of cytologic atypia, the abundance of mitotic figures, and the presence or absence of visible intercellular bridges, keratin pearls (aggregates of anucleate keratin), and necrosis.
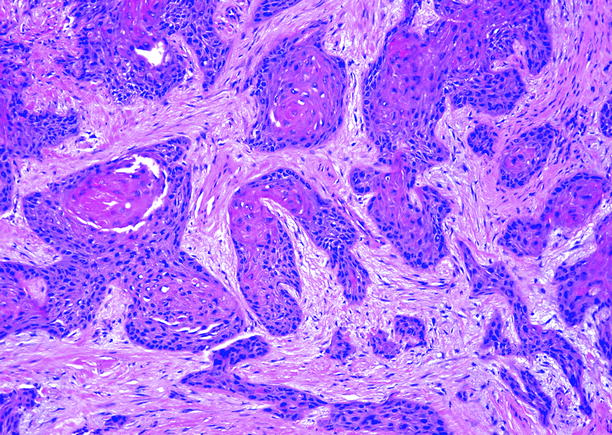
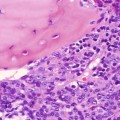
Fig. 9.4
Squamous cell carcinoma, conventional type. Squamous cell carcinoma of conventional type is typically well or moderately differentiated, composed of irregular fingers and nests of malignant squamous cells that infiltrate underlying tissues. Stromal desmoplasia and infiltrates of chronic inflammatory cells are commonly present. Keratin pearls are present
Well-differentiated squamous cell carcinoma has minimal cytologic atypia, rare mitotic figures, abundant keratin pearls, and readily visible intercellular bridges. It often forms papillomatous exophytic structures and infiltrates underlying tissues as delicate fingerlike projections.
Poorly differentiated carcinoma exhibits abundant mitotic figures, absence of recognizable intercellular bridges, absence of keratin pearls, and pronounced nuclear atypia. Necrosis may be present.
The features of moderately differentiated carcinoma are intermediate between these extremes; intercellular bridges and keratin pearls are present but infrequent, and mitotic activity and nuclear atypia are greater than in well-differentiated tumors, but less than in poorly differentiated tumors.
As the degree of differentiation diminishes, the likelihood of lymph node metastases increases and the prognosis worsens (Fig. 9.5). Lymph node metastases occur in about 25 % of patients with well-differentiated cancer, in nearly half with moderately differentiated carcinoma, and in over 80 % of patients with poorly differentiated carcinoma.

Fig. 9.5
Squamous cell carcinoma. Clinical photo showing massively enlarged inguinal lymph nodes involved by metastatic cancer
Penile squamous cell carcinoma tends to follow various growth patterns, which also correlate with the incidence of lymph node metastases and the prognosis. Those that grow vertically are often high grade and deeply invasive. Superficial spreading carcinomas are usually well or moderately differentiated, grow horizontally, and invade minimally. Invasion by verruciform carcinomas is limited or nonexistent. Over 80 % of vertical growth carcinomas develop inguinal lymph node metastases, whereas node metastases in the other growth patterns occur in fewer than half the cases. Prognosis is best for patients with verruciform cancers, worst for those with vertical growth tumors, and intermediate between these extremes for patients with superficial spreading tumors.
Other Penile Tumors
Imaging Findings
Ultrasound
Giant cavernous hemangioma appears as a heterogeneously echogenic mass with multiple hypoechoic lacunae. The lesion may spread in the soft tissues outside the penile bodies, involving the scrotum and the perineum for a variable extent (Fig. 9.6a, b), or involve also portions of the corpus spongiosum and of the corpora cavernosa. No vascularization is usually appreciable at color flow Doppler interrogation.
Fig. 9.6
A 24-year-old patient with giant penoscrotal hemangioma. (a) Axial ultrasound scan on the ventral aspect of the penile shaft reveals a heterogeneous thickening of the dorsal extraalbugineal tissues (curved arrows) with anechoic lacunae. CC corpora cavernosa, CS corpus spongiosum. (b) Longitudinal ultrasound scan of the scrotum demonstrates heterogeneous extratesticular tissue with similar appearance (curved arrow) displaying no vascular signal at color Doppler interrogation. (c) T1-weighted sagittal MR image showing thickening of the superficial tissues in the dorsal aspect of the penis (arrows), and a lobulated extratesticular mass of intermediate signal intensity in the scrotum (*). (d) The T2-weighted sagittal MR image better delineates the hyperintense penoscrotal lesion which widely involves the dorsal aspect of the penis (arrows), the glans (arrowheads), and the scrotum (*) and extends also in the perineum (curved arrow)
Neurilemmoma presents as a well-defined, hypoechoic rounded, highly vascularized mass.
Schwannoma may present as a heterogeneous extracorporeal mass with well-defined margins.
Epithelioid sarcoma may present as a solid mass with multiple focal calcifications infiltrating the corpora cavernosa.
Kaposi’s sarcoma usually presents as a heterogeneously hypoechoic vascularized mass with ill-defined margins.
Lymphoma presents as an isoechoic or relatively hypoechoic hypervascularized lesion often with infiltration of the corpora cavernosa.
Computed Tomography
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


