Chapter 6 Etiologies, Pathophysiology, and Clinical Presentation: The orbital septum, the anterior reflection of the periosteum of the orbital wall onto the tarsal plate of the eyelid, divides the orbit into preseptal and postseptal compartments. Periorbital cellulitis refers to infection anterior to the orbital septum involving the eyelid and adnexa. Orbital cellulitis refers to infection posterior to the orbital septum. This distinction is important because orbital cellulitis carries the risks of abscess, blindness, venous thrombosis, intracranial extension, and death. Defects in the orbital septum, direct extension from sinus infection, and valveless veins provide infection with access to the postseptal orbit. Sinusitis is the most common cause (60% to 85%), with stye, dacryoadenitis/cystitis, dental abscess, skin breaks, and hematogenous seeding being less common.1,2 Staphylococcus aureus, S. epidermidis, and S. pyogenes account for ~75% of infections; rates of Hemophilus influenzae and streptococcal pneumonia are declining as a result of immunization.1 Patients present with erythema, swelling, warmth, and tenderness of the eyelid. Although ophthalmoplegia and proptosis predict postseptal involvement and abscess, approximately 50% of patients with an abscess do not have these symptoms. As a result, the guidelines for imaging are unclear and vary: edema preventing a complete examination, signs of central nervous system involvement, deteriorating vision, proptosis, ophthalmoplegia, and/or deterioration after 24 to 48 hours of treatment.3–5 Imaging: Periorbital cellulitis presents with eyelid swelling and thickening of the preseptal soft tissues on computed tomography (CT), with T2 hyperintensity on magnetic resonance imaging (MRI) (Fig. 6-1, A).2,6,7 In orbital cellulitis, similar inflammatory changes of the extraconal and/or intraconal orbital fat are present. The most common complication of orbital cellulitis is subperiosteal abscess, frequently involving the lamina papyracea, and directly extending from ethmoid sinus disease. A subperiosteal abscess presents as a broad-based, peripherally enhancing fluid collection along the medial wall of the orbit that displaces the medial rectus muscle laterally (Fig. 6-2, A). Less commonly, an abscess can form in the extraconal or intraconal orbit separate from the bone, which also is seen as a peripherally enhancing fluid collection. MRI can be helpful in identifying an abscess by demonstrating restricted diffusion.8 Figure 6-1 Periorbital cellulitis. Figure 6-2 Orbital cellulitis. Treatment: Treatment consists of oral antibiotics covering staphylococcus and streptococcus for periorbital cellulitis and admission to the hospital with administration of intravenous (IV) antibiotics for orbital cellulitis. Surgical intervention for drainage of an abscess is required in only 12% of admitted patients,3 and an orbital abscess can be treated with IV antibiotics if it is small or appears in a young child.9,10 Dacryocystitis is the result of bacterial overgrowth of stagnant fluid in the nasolacrimal sac presenting with epiphora, erythema, and edema at the medial canthus. In neonates, dacryocystitis can complicate 33% to 65% of cases of congenital dacryocystocele caused by incomplete canalization of the distal nasolacrimal duct.11,12 In older children, dacryocystitis can result from other causes of nasolacrimal duct obstruction, including rhinitis/sinusitis, tumor, or trauma and fracture. CT or MRI demonstrates a cystic medial canthus mass with adjacent inflammatory changes (Fig. 6-1, B).13–15 Although infection is most commonly associated with periorbital cellulitis, it rarely can extend into the postseptal orbit with abscess formation.16 Treatment typically consists of antibiotics and dacryocystorhinostomy. Superior ophthalmic vein (SOV) thrombosis is a complication of orbital cellulitis that results from inflammatory thrombophlebitis or direct venous invasion by infection; 33% to 75% of isolated SOV thrombosis leads to cavernous sinus thrombosis, which carries a mortality rate of 20%.17,18 Imaging with CT or MRI demonstrates an enlarged S-shaped SOV below the superior rectus muscle with a filling defect and peripherally enhancing vasa vasorum on postcontrast images (Fig. 6-2, B).19 Restricted diffusion of the SOV also has been reported, facilitating identification.20 Treatment consists of aggressive use of antibiotics with or without corticosteroids and anticoagulation, which are not proven therapies.17,18 Ocular toxocariasis refers to infection of the globe by the nematodes Toxocara canis or Toxocara cati. It is one of several ocular infections caused by parasitic worms, including onchocerciasis (Onchocerca volvulus), cysticercosis (Taenia solium), and diffuse unilateral subacute neuroretinitis. Ocular toxocariasis is most common in the southeastern United States in children 6 to 12 years of age as a result of ingestion of food or soil contaminated by the feces of dogs or cats. It presents with painless unilateral vision loss, strabismus, and leukocoria.21 CT and MRI demonstrate an intravitreal enhancing mass with or without adjacent uveoscleral thickening and retinal detachment. A normal-sized globe containing a mass without calcification differentiates toxocariasis from other common causes of leukocoria (e.g., retinoblastoma, persistent hyperplastic primary vitreous, Coats disease, and retinopathy of prematurity).22,23 Etiologies, Pathophysiology, and Clinical Presentation: Orbital pseudotumor (OP) is a noninfectious inflammatory condition of the orbit of unclear etiology. In adults it is the most common painful orbital mass, accounting for ~10% of orbital masses, and is the third most common orbital disease. Pediatric OP is rare, with only 68 cases reported in the medical literature as of 2008, accounting for only 7% to 16% of cases of OP.24,25 Children present similarly to adults with pain, proptosis, a mass, swelling, and motility restriction; however, children more frequently demonstrate ptosis and bilateral or intraocular involvement. Imaging: Both CT and MRI are useful in evaluating OP.26–28 Lacrimal gland involvement is most common, with enlargement and adjacent inflammatory change. Myositis also occurs frequently, typically with unilateral tubular thickening of extraocular muscles and tendons (compared with Graves orbitopathy, which tends to be bilateral with tendon sparing). OP may involve the uvea and sclera with thickening and enhancement (Fig. 6-3, A). Perineuritis, which involves the optic nerve sheath, demonstrates “tramline” inflammatory changes and enhancement surrounding the optic nerve (Fig. 6-3, B-D). Inflammation can extend through the orbital fissures and optic canal into the cavernous sinus and middle cranial fossa. The differential diagnosis includes infection, lymphoma, Wegener granulomatosis, sarcoidosis, and Graves orbitopathy. Diffusion-weighted imaging may be helpful in the diagnosis with the intensity of lymphoid lesions > OP > cellulitis on b-value = 1000 images.29 Figure 6-3 Orbital pseudotumor. Treatment: Administration of oral corticosteroids often results in a rapid response (within 1 to 2 days); radiation is used in refractory cases.25,30 Recurrence after withdrawal of steroids occurs frequently in adults (~50%) but has been reported in only one child.24,31 Biopsy is reserved for atypical symptoms or poor response. Recently, cases of OP have been identified as part of IgG4-related disease, a systemic inflammatory disease demonstrating excellent response to rituximab and corticosteroids.32,33 Etiologies, Pathophysiology, and Clinical Presentation: Graves orbitopathy is an orbital inflammatory process seen in persons with Graves disease, which is an autoimmune thyroid disease from thyroid-stimulating hormone receptor autoantibodies. Pediatric Graves disease is uncommon, yet children who have the disease experience Graves orbitopathy at similar rates as do adults, in one third to two thirds of cases.34–36 Graves orbitopathy is milder in children than in adults, with mild proptosis and mild eyelid retraction or lag. In children, no cases of compressive optic neuropathy have been reported, and strabismus is rare. Imaging: Imaging demonstrates fusiform enlargement of extraocular muscles (involving muscle bellies and sparing tendons), which is bilateral in 90% of cases and frequently involves the inferior and medial recti. Increased volume of orbital fat and lacrimal gland enlargement also can be seen.37 Active disease can be differentiated from fibrotic disease by evaluating the T2 signal intensity and dynamic contrast enhancement of the muscles (T2 hyperintensity, shorter time to peak, and greater enhancement and washout ratios are found in persons with active disease). This distinction is important, because medical therapy is not effective in persons with fibrotic disease.38–40 Sarcoidosis is a multisystem disease of unclear etiology characterized by noncaseating granulomas. Sarcoidosis is rare in children; however, a unique form appears in children younger than 5 years and presents with rash, uveitis, and arthritis.41 In older children and adults, ocular involvement is seen in ~25% of cases, most commonly with uveitis.41–44 Additional orbital structures involved can include the lacrimal gland and sac, eyelid, orbital soft tissues, optic nerve and sheath, and extraocular muscles, with enlargement and enhancement of these structures.45,46 Involvement can be well circumscribed (in 85% of cases) or diffuse (in 15% of cases). The mainstay of treatment is oral steroids, which generally results in a good response; methotrexate or surgery is used for refractory cases. In patients with isolated orbital involvement (63%), systemic disease develops in 8% within 5 years.47 Wegener granulomatosis is a necrotizing granulomatous vasculitis of small and medium-sized vessels associated with antineutrophil cytoplasmic antibodies. Pediatric Wegener granulomatosis is rare; it presents in adolescence with a female predominance.48,49 Orbital involvement occurs in approximately 50% of adults (and is the presenting feature in 15%), but it is less common in children.50,51 Orbital disease may be primary or extend from the sinuses with osseous erosion. The globe (conjunctivitis and scleritis), lacrimal gland, retrobulbar space, optic nerve, and extraocular muscles all can be involved. Imaging demonstrates granulomatous masses with variable enhancement and characteristic T2-weighted hypointensity on MRI, presumably related to fibrocollagenous tissue (Fig. 6-4).52,53 Visual impairment related to optic nerve compression or vasculitis is seen in up to 20% to 50% of adults. Nasolacrimal duct obstruction from sinus disease can result in dacryocystitis. Treatment in children can vary but typically consists of administration of steroids and cyclophosphamide. Figure 6-4 Wegener granulomatosis. Etiologies, Pathophysiology, and Clinical Presentation: Optic neuritis (ON) is an inflammatory disease of the optic nerve with acute onset of vision loss and periocular pain (in >90% of adults). ON may be idiopathic or related to multiple sclerosis (MS), neuromyelitis optica, or acute disseminated encephalomyelitis. ON behaves differently in children than in adults, likely reflecting different etiologies, with parainfectious ON being common in children (in one third to two thirds of cases).54–58 Compared with adults, ON in children is more often bilateral (in 37% to 66% of cases), less often painful (in 37% of cases), and more often demonstrates disk swelling (in 46% to 85% of cases) and profound vision loss. In children it tends to have better visual recovery and is less often associated with MS. Imaging: MRI demonstrates contrast enhancement (>90%), T2-weighted hyperintensity, and mild enlargement of the optic nerves acutely, with mild volume loss developing chronically (Fig. 6-5).59,60 If frank enlargement of the optic nerve is seen, an optic pathway glioma should be considered. Intraorbital involvement is most common. Intracanalicular and long segment involvement and persistent signal change over time correlate to worse visual outcomes. Retinal nerve fiber layer thinning on optical coherence tomography also correlates to vision loss.61,62 Diffusion tensor imaging of optic nerves is difficult perform clinically, yet demonstrates decreased axial diffusivity acutely and increasing radial diffusivity and apparent diffusion coefficient values during recovery, correlating to changes in visual acuity and retinal nerve fiber layer thinning.63–65 Decreased fractional anisotrophy values also can be seen in the optic tracts and radiations, possibly as a result of Wallerian and transsynaptic degeneration.66–68 Magnetization transfer ratios (MTRs), which are thought to decrease with demyelination, are more sensitive than T2 spin echo imaging. They progressively decrease in the optic nerve, with a nadir at 240 days, and then mildly increase (possibly from remyelination), also correlating to changes in visual acuity.69,70 Figure 6-5 Optic neuritis.
Orbit Infection and Inflammation
Periorbital and Orbital Cellulitis
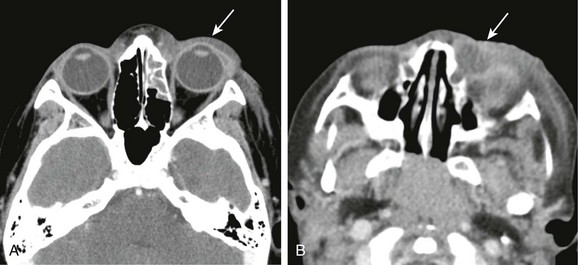
A, A computed tomography (CT) image of periorbital cellulitis from adjacent sinusitis demonstrates preseptal soft tissue swelling (arrow). B, A CT image of dacryocystitis causing periorbital cellulitis demonstrates a cystic medial canthus mass (arrow) with adjacent inflammatory changes.
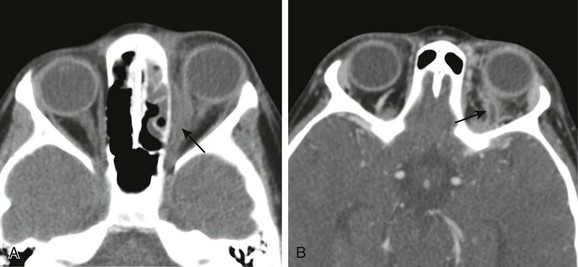
A, A computed tomography (CT) scan of orbital cellulitis with a subperiosteal abscess demonstrates inflammatory changes of the fat of the postseptal orbit with a broad-based, peripherally enhancing fluid collection adjacent to the lamina papyracea (arrow). B, A CT scan of superior ophthalmic vein (SOV) thrombosis demonstrates an enlarged S-shaped SOV with a filling defect and peripheral enhancement (arrow).
Dacryocystitis
Superior Ophthalmic Vein Thrombosis
Ocular Toxocariasis
Orbital Pseudotumor (Idiopathic Orbital Inflammation)
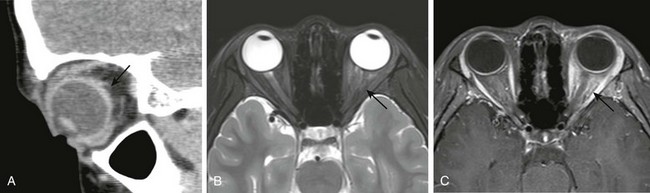
A, A sagittal computed tomography image of scleral involvement by a pseudotumor causing posterior scleritis with subtle thickening of the posterior sclera (arrow). B, A T2-weighted fat-saturated magnetic resonance image in a different patient with a pseudotumor demonstrating ill-defined T2 hyperintensity of the intraconal fat (arrow). C, A T1-weighted fat-saturated postcontrast image demonstrating corresponding “tramline” enhancement of the optic nerve sheath and ill-defined enhancement of the intraconal fat (arrow).
Graves Orbitopathy (Thyroid Orbitopathy)
Sarcoidosis
Wegener Granulomatosis
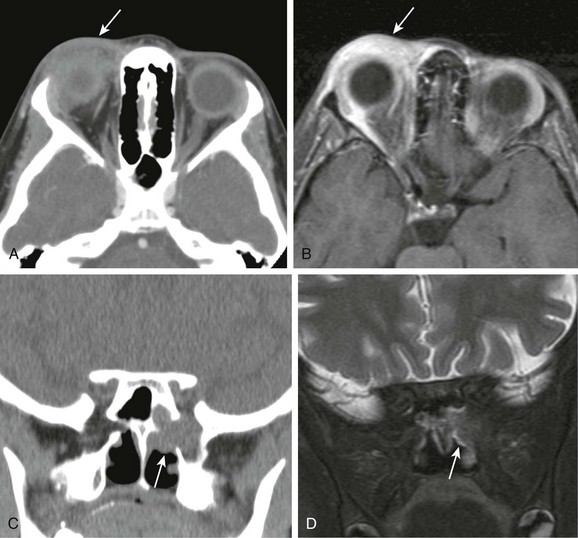
A and B, Computed tomography (CT) and T1-weighted fat-saturated postcontrast magnetic resonance (MR) images of the orbit demonstrating inflammatory changes and enhancement adjacent to the lacrimal gland in the preseptal orbit, similar in appearance to periorbital cellulitis (arrow). C and D, Coronal CT and T2-weighted fat-saturated MR images demonstrating a mass centered on the sphenopalatine foramen with osseous erosion and extension to the orbital apex with characteristic T2 hypointensity, making it difficult to visualize on MR imaging (arrows).
Optic Neuritis
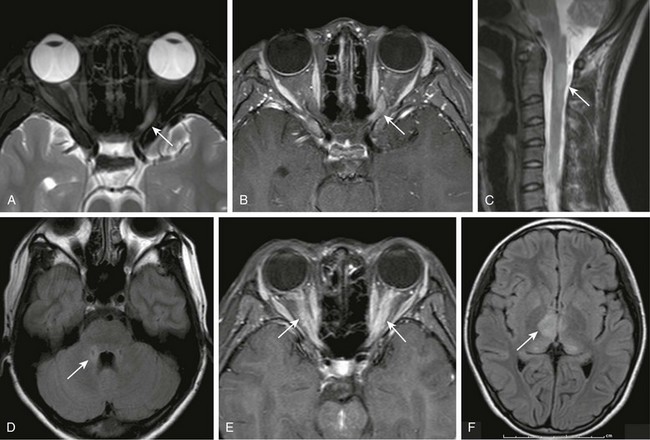
T2- (A) and T1-weighted fat-saturated postcontrast (B) magnetic resonance (MR) images of the orbits demonstrating abnormal T2 hyperintensity and enhancement of the left optic nerve (arrows). C, A sagittal T2-weighted MR image of the cervical spine demonstrates a characteristic central long segment cord lesion in a patient with neuromyelitis optica (NMO) (arrow). D,Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree