and Jurgen J. Fütterer2, 3
(1)
Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Rome, Italy
(2)
Department of Radiology and Nuclear Medicine, Radboudumc, Nijmegen, The Netherlands
(3)
MIRA Institute for Biomedical Technology and Technical Medicine, University of Twente, Enschede, The Netherlands
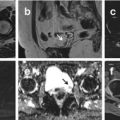
Pelvic Inflammatory Disease
Pelvic inflammatory disease (PID) is a common condition among women of reproductive age and is usually caused by infection ascending from the endocervix through the uterine cavity.
Patients usually present with a myriad of nonspecific symptoms, including fever, abdominal or pelvic pain, vaginal discharge, uterine bleeding, dyspareunia, dysuria, adnexal or cervical tenderness, nausea, vomiting, and other vague constitutional symptoms. Laparoscopy, which allows direct visualization of purulent exudates and edema of the pelvic structures, has long been the standard of reference in the diagnosis of PID, but it requires general anesthesia and is an expensive and invasive procedure.
CT: CT findings are typically subtle early in the course of PID. Mild pelvic edema that results in thickening of the uterosacral ligaments and haziness of the pelvic fat with obscuration of the pelvic fascial planes are seen in the initial phase. Later in the course of PID, the fallopian tubes exhibit an even greater degree of wall thickening and enhancement and fill with complex fluid, findings that usually indicate pyosalpinx. The abscess manifests as bilateral thick-walled, fluid-filled adnexal masses. The abscess wall and adjacent soft tissue inflammation enhance intensely. Internal gas bubbles, which are unusual, are the most specific sign of an abscess.
MRI: Tubal enlargement can be easily seen on MR images and is characterized by the tortuous folding of fluid-filled structures on T2-weighted images. Associated findings include thickening of the uterosacral ligaments, infiltration of the presacral fat secondary to edema, hydronephrosis, and indistinct margins of adjacent bowel loops.
Penis Prosthesis
Penis prosthesis is a treatment option for men with erectile dysfunction. There are two main types of penile implants: semi-rigid and inflatable.
MRI can clearly demonstrate the position of both semirigid and inflatable prostheses. The saline solution in inflatable devices is well seen with T2-weighted sequences; the silicone in semirigid devices has low signal intensity on T2-weighted images.
Peyronie Disease
Peyronie disease is a common acquired condition, with a prevalence of around 3 %, associated with penile curvature and a palpable plaque in the tunica albuginea and adjacent corpus cavernosum. The plaque is mostly located unifocally in the penile dorsum with an extension of about 1.5–3 cm causing a typical dorsal deviation. Morphologically, an inflammatory reaction with thickening of the tunica in the beginning, later on a fibrotic, often calcified plaque is typical.
Plaques from Peyronie disease are usually palpable and are visible at both US and MR imaging in the majority of cases.
CT is not routinely used and can only show calcification.
MRI: Plaque formation has been associated with low signal intensity, disruption, localized thickening, and irregularity of the adjacent tunica albuginea with both T1- and T2-weighted sequences. Erection induced by the injection of Prostaglandin E1 stretches the tunica albuginea improving the conditions for plaque detection. The intravenous application of paramagnetic contrast medium leads to an increased local signal intensity (T1-weighted) depending on the degree of tissue perfusion with a focal contrast enhancement around or within the plaques indicating an inflammatory status of the plaque.
Polycystic Kidney Disease
The Potter classification of renal cystic diseases separates cystic kidneys into four types: (1) infantile polycystic kidney disease; (2) cystic dysplastic kidney disease; (3) adult polycystic kidney disease; and (4) partial or intermittent urinary outflow obstruction (obstructive dysplasia).
Autosomal Recessive Polycystic Kidney Disease (ARPKD): also known as Potter type I and infantile polycystic disease, the autosomal-recessive form of polycystic kidney disease manifests early in life. The underlying defect is renal tubular ectasia. The nephrons are normal. Expressivity varies with some patients not surviving beyond the neonatal period. Those with milder renal involvement survive longer and develop hepatobiliary fibrosis and dilated bile ducts. In the infantile form, numerous small cysts (several millimeter range) develop throughout, the kidneys are markedly enlarged, poor function is evident early on, and renal failure gradually ensues.
CT: CT reveals renal cysts to be near water density unless superimposed bleeding occurs.
MRI: Renal cysts appear rounded well-defined structures with very thin regular walls; these cysts vary from hypo- to hyperintense both with T1- and T2-weighted images, presumably due to prior hemorrhage.
Autosomal Dominant Polycystic Kidney Disease (ADPKD): also called adult polycystic kidney disease and Potter type III, is the most common hereditary renal disorder. Renal failure is a late finding. These patients are also prone to developing aortic and cerebral aneurysms with their related complications.
Clinical presentation is variable and includes dull flank pain of variable severity and time course: most common, abdominal/flank masses, hematuria, and hypertension.
CT: CT shows most cysts to resemble simple cysts, although hemorrhage into cysts is common and these are hyperdense to water. The walls are very thin and regular and are often imperceptible. Some have a fluid–fluid level or even appear as a solid tumor. Renal calcifications are generally secondary to calculi, prior hemorrhage into a cyst, or cyst wall calcifications.
MRI: Renal cysts appear rounded well-defined structures with very thin regular walls; these cysts vary from hypo- to hyperintense both with T1- and T2-weighted images, presumably due to prior hemorrhage.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree