21 Positron emission tomography (PET) can be useful in differentiating benign pancreatic masses from adenocarcinoma.
Pancreatic Cancer
Eugene C. Lin and Abass Alavi
 Pancreatic Masses and Adenocarcinoma
Pancreatic Masses and Adenocarcinoma
Clinical Indication: B
Accuracy and Comparison with Other Modalities
Sensitivity %
Specificity %
PET
92
85
CT
65
62
Pearls
- Clinical history4
- The absence of clinical and laboratory findings of acute pancreatitis does not rule out an inflammatory etiology for a pancreatic mass.
- Obtaining a C-reactive protein may be helpful, as false-positive results due to inflammation are more likely to occur when C-reactive protein is elevated.
- The absence of clinical and laboratory findings of acute pancreatitis does not rule out an inflammatory etiology for a pancreatic mass.
- Characteristics of malignant versus inflammatory masses
- Inflammatory lesions are often more diffuse than focal.
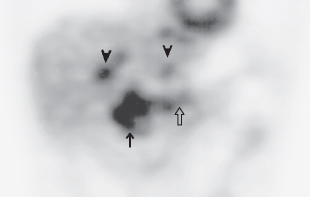
- However, acute or chronic pancreatitis secondary to duct obstruction can be seen in conjunction with pancreatic malignancy. In these cases, it is difficult to distinguish tumor from pancreatitis on PET (Fig. 21.1).
- Although chronic pancreatitis can cause false-positive results, the majority (87%) of patients with chronic pancreatitis have negative PET exams. The possibility of malig nancy should still be pursued in patients with chronic pancreatitis and positive PET.5
- Inflammatory lesions are often more diffuse than focal.
- Standardized uptake values (SUV)
- There is no generally agreed upon SUV cutoff for differentiating benign from malignant lesions: published values range from 2.0 to 4.0.6,7
- If the patient has a history of pancreatitis, using SUV cutoff in the higher range helps to avoid false-positive results because pancreatic inflammatory lesions can have substantial uptake.
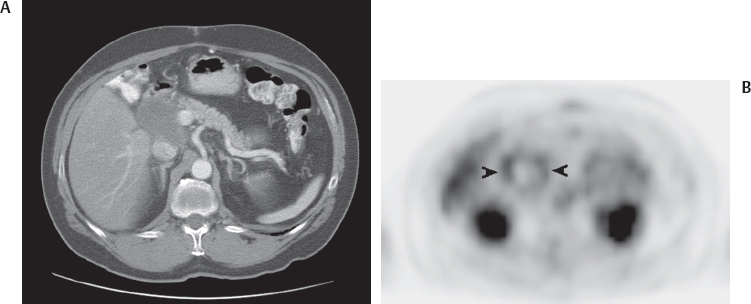
Fig. 21.2 Pancreatic pseudocyst. (A) Computed tomography scan demonstrates a cystic lesion in the pancreatic head region. (B) Axial positron emission tomography scan at a slightly more inferior level demonstrates uptake around the cyst (arrowheads) but no uptake within the cyst. This appearance is consistent with a pseudocyst.
Table 21.2 Sensitivity and Specificity of Positron Emission Tomography/Computed Tomography (PET/CT) versus Computed Tomography in the Detection of Malignant Cystic Pancreatic Tumors
Sensitivity %
Specificity %
PET/CT
86
91
CT
67 to 71
87 to 90
- SUV values should be corrected for glucose level if possible.
- There is no generally agreed upon SUV cutoff for differentiating benign from malignant lesions: published values range from 2.0 to 4.0.6,7
- Delayed imaging8
- Delayed imaging at 2 hours can help differentiate between malignant lesions and benign inflammatory lesions.
- Malignant lesions will have increasing uptake over time, whereas inflammatory lesions will have a decline in uptake.
- However, 19% of malignant pancreatic tumors show a decline in uptake from 1 to 2 hours.9
- Delayed imaging at 2 hours can help differentiate between malignant lesions and benign inflammatory lesions.
Pitfalls
- Hyperglycemia. Hyperglycemia is a confounding factor for all oncologic PET but is the most problematic in pancreatic PET, where it causes a high false-negative rate. PET must be interpreted with caution in hyperglycemic patients with a pancreatic mass.
- False-positives. Pancreatitis (chronic, acute, autoimmune), benign lesions (serous cystadenoma, hemorrhagic pseudocyst)
- False-negatives. Early-stage tumors, elevated glucose
 Cystic Tumors
Cystic Tumors
Clinical Indication: C
- Accuracy. PET or PET/CT can differentiate benign from malignant cystic tumors (Fig. 21.2) with greater accuracy than CT, using an SUV cutoff of 2.5 (Table 21.2).11,12
- Intraductal papillary mucinous tumor (IPMT). IPMT usually has increased fluorodeoxyglucose (FDG) uptake.13,14
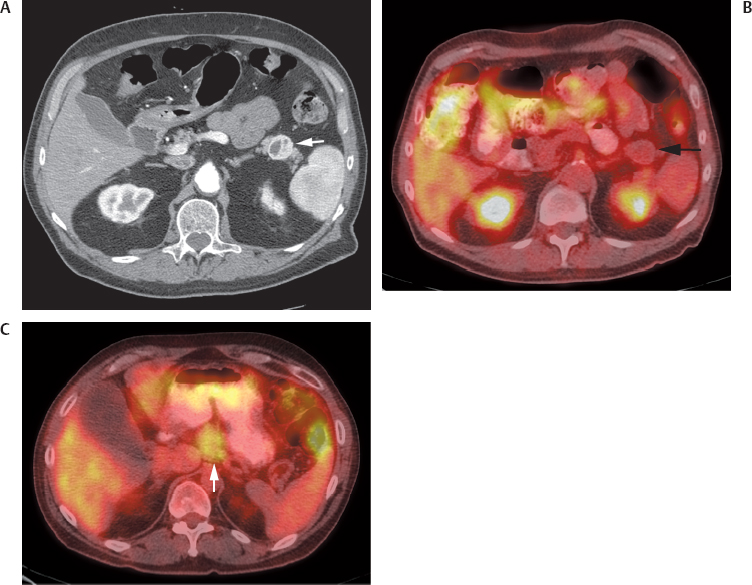
Fig. 21.3 Pancreatic islet cell tumors with variable fluorodeoxyglucose (FDG) uptake. (A) Axial computed tomography (CT) scan demonstrates a hypervascular islet cell tumor in the tail of the pancreas (arrow). (B) Axial positron emission tomography (PET)/CT scan demonstrates lack of FDG uptake in the islet cell tumor (arrow). (C) Axial PET/CT scan in another patient demonstrates moderate FDG uptake in an islet cell tumor (arrow) arising from the body of the pancreas.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree





