Can be solitary (73%), multiple (10%), or diffusely infiltrative (15%)
Enhancement pattern mimics primary tumor
– Hypervascular: Most commonly renal cell cancer (RCC)
– Hypovascular: Lung, breast, colon, melanoma
Concomitant intraabdominal metastases in > 60%, usually with widespread metastatic disease
• Pancreatic lymphoma
Homogeneous soft tissue mass with little enhancement
Diffuse enlargement of pancreas with infiltrating tumor (± peripancreatic fat involvement) may mimic acute pancreatitis
Almost always associated lymphadenopathy or other sites of lymphomatous involvement
Tumor classically encases peripancreatic vessels without narrowing or occlusion
No dilatation of pancreatic duct or biliary tree
TOP DIFFERENTIAL DIAGNOSES
• Pancreatic ductal carcinoma
Usually focal hypodense mass that obstructs main pancreatic duct resulting in upstream ductal dilatation
Encases and narrows peripancreatic vessels
• Pancreatic islet cell tumors
Usually hypervascular lesions which are indistinguishable from RCC metastases without clinical history
CLINICAL ISSUES
• Prognosis of metastases to pancreas poor, although isolated metastases to pancreas may be amenable to resection (especially RCC)
RCC metastases to pancreas may occur 5-10 years after primary tumor resection
• Prognosis for primary pancreatic lymphoma is poor, with 30% cure rate after treatment
(Left) Axial CECT shows a hypodense mass in the pancreatic tail due to metastatic sarcoma. Metastases from lung, breast, colon, or melanoma could have a similar appearance.
(Right) Coronal MIP reconstruction of an arterial phase CECT demonstrates an avidly enhancing pancreatic mass in a patient with a history of prior nephrectomy for renal cell carcinoma (RCC), a characteristic appearance for an RCC metastasis. Based on appearance alone, this mass is indistinguishable from a neuroendocrine tumor.
(Left) Axial T1WI C+ MR shows an enhancing RCC metastasis in the pancreatic head. The pancreatic duct is mildly dilated upstream. Note the posterior position of the pancreatic tail as a result of a prior left nephrectomy for RCC several years prior to this scan.
(Right) Axial CECT shows diffuse infiltration of the pancreas and invasion of the spleen by non-Hodgkin lymphoma. Also note the associated peripancreatic lymphadenopathy .
IMAGING
General Features
• Best diagnostic clue
Mass(es) in pancreas, usually without pancreatic or biliary ductal obstruction
CT Findings
• Pancreatic metastases
May be solitary (73%), multiple (10%), or diffusely infiltrative (15%)
Enhancement pattern is variable, but typically mimics primary tumor
– Hypervascular: Most often renal cell cancer (RCC)
– Hypovascular: Lung, breast, melanoma, colon
Concomitant intraabdominal metastases in 60-95%, usually with widespread metastatic disease
– Liver, nodes, adrenal (each ∼ 30%)
Dilatation of pancreatic duct or bile ducts less common than pancreatic adenocarcinoma (40%)
Encasement or narrowing of peripancreatic vasculature is unusual
• Pancreatic lymphoma
Most often presents as discrete homogeneous soft tissue mass with little enhancement
May rarely present as diffuse enlargement of pancreas with infiltrating tumor ± peripancreatic fat involvement
– Infiltrating tumor may mimic acute pancreatitis
Almost always associated with lymphadenopathy (especially peripancreatic) and other sites of lymphomatous involvement
Tumor classically encases peripancreatic vasculature without narrowing or occlusion
No dilatation of pancreatic duct or biliary tree
No upstream atrophy of pancreatic parenchyma
Only gold members can continue reading. Log In or Register to continue


 Diffuse enlargement of pancreas with infiltrating tumor (± peripancreatic fat involvement) may mimic acute pancreatitis
Diffuse enlargement of pancreas with infiltrating tumor (± peripancreatic fat involvement) may mimic acute pancreatitis








 in the pancreatic tail due to metastatic sarcoma. Metastases from lung, breast, colon, or melanoma could have a similar appearance.
in the pancreatic tail due to metastatic sarcoma. Metastases from lung, breast, colon, or melanoma could have a similar appearance.
 in a patient with a history of prior nephrectomy for renal cell carcinoma (RCC), a characteristic appearance for an RCC metastasis. Based on appearance alone, this mass is indistinguishable from a neuroendocrine tumor.
in a patient with a history of prior nephrectomy for renal cell carcinoma (RCC), a characteristic appearance for an RCC metastasis. Based on appearance alone, this mass is indistinguishable from a neuroendocrine tumor.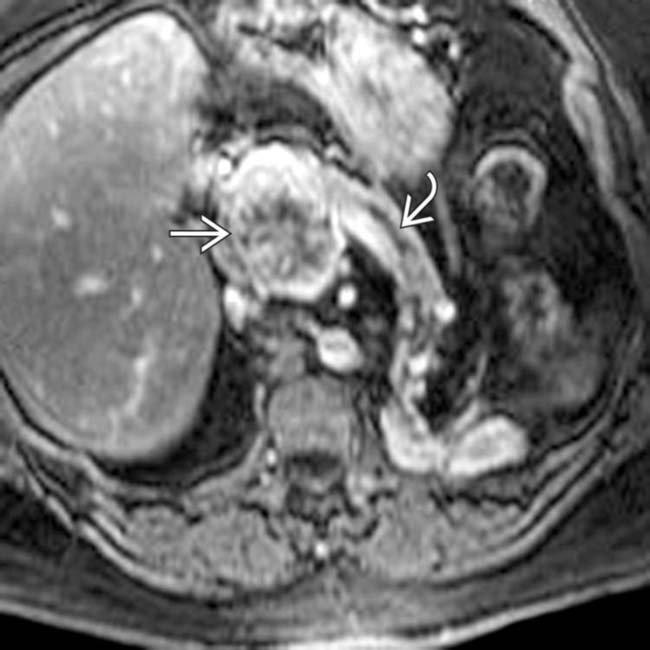
 in the pancreatic head. The pancreatic duct
in the pancreatic head. The pancreatic duct  is mildly dilated upstream. Note the posterior position of the pancreatic tail as a result of a prior left nephrectomy for RCC several years prior to this scan.
is mildly dilated upstream. Note the posterior position of the pancreatic tail as a result of a prior left nephrectomy for RCC several years prior to this scan.
 by non-Hodgkin lymphoma. Also note the associated peripancreatic lymphadenopathy
by non-Hodgkin lymphoma. Also note the associated peripancreatic lymphadenopathy  .
.





 May rarely present as diffuse enlargement of pancreas with infiltrating tumor ± peripancreatic fat involvement
May rarely present as diffuse enlargement of pancreas with infiltrating tumor ± peripancreatic fat involvement Almost always associated with lymphadenopathy (especially peripancreatic) and other sites of lymphomatous involvement
Almost always associated with lymphadenopathy (especially peripancreatic) and other sites of lymphomatous involvement








