Most often solid, but can have variable internal cystic components and intratumoral hemorrhage
• Capsule enhances on CECT and T1 C+ MR and appears as rim of low T2 signal intensity
• Frequent peripheral or central calcification (45-50%)
• Presence of internal hemorrhage highly characteristic feature, and may result in fluid-fluid or hematocrit levels
Internal hemorrhage usually easier to perceive on MR
• Usually no biliary or pancreatic ductal obstruction
• Metastatic disease is very uncommon, but most often metastasizes to liver and locoregional lymph nodes
PATHOLOGY
• Rare: < 3% of all pancreatic tumors
• Previously thought to have separate benign and malignant subtypes, but recent WHO classification defines all SPEN as low-grade malignancies
Low malignant potential (< 10% metastasize or recur)
CLINICAL ISSUES
• > 90% occur in women
• Almost always arises in patients < 35 years (rarely reported in older adults)
Accounts for 8-16% of pancreatic tumors in children
• Possible predilection for African Americans and Asians
• Most patients are symptomatic, with abdominal pain most common presenting symptom
• Treatment: Complete surgical resection
DIAGNOSTIC CHECKLIST
• Consider SPEN when confronted by an encapsulated solid pancreatic mass in a young woman, particularly when there is evidence of internal hemorrhage
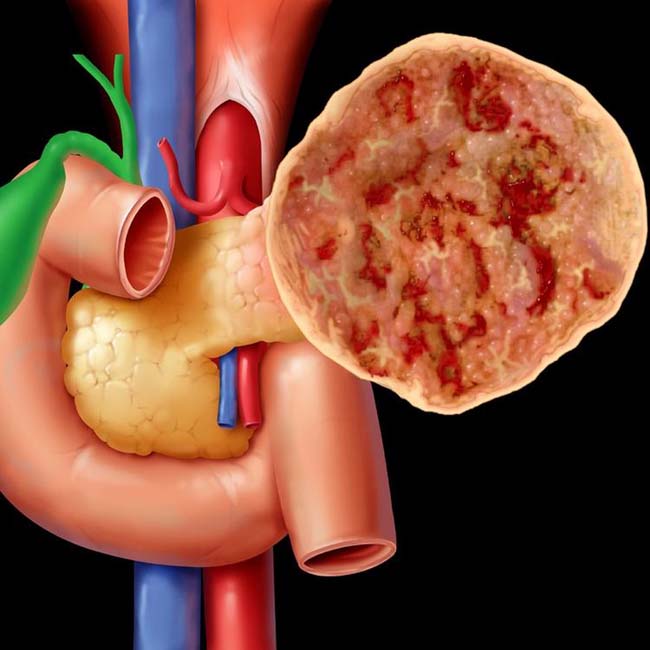
(Left) Graphic shows a large encapsulated mass arising from the pancreatic tail with prominent solid and cystic or hemorrhagic components.
(Right) Axial CT in 42-year-old man with an incidentally discovered pancreatic mass demonstrates a well-circumscribed, predominantly cystic mass in the pancreatic body with a clearly visible enhancing capsule. The mass was found to be a solid pseudopapillary neoplasm (SPEN) at surgery.
(Left) Axial CT in a 21-year-old woman shows a complex cystic-solid mass with peripheral rim calcification in the tail of the pancreas. Endoscopic ultrasound (not shown) confirmed a complex cystic mass. Needle aspiration of the mass at ultrasound yielded fluid that had few cells and no elevated tumor markers. The fluid was not mucoid.
(Right) The resected mass shows areas of hemorrhage and necrosis, surrounded by tissues with solid and pseudopapillary projections , compatible with a SPEN.
TERMINOLOGY
Abbreviations
• Solid and pseudopapillary neoplasm (SPEN)
Synonyms
• Hamoudi tumor, Franz tumor
• Papillary epithelial neoplasm, papillary cystic carcinoma, solid and cystic tumor of pancreas, Franz tumor, solid and papillary epithelial neoplasm,
IMAGING
General Features
• Best diagnostic clue
Encapsulated solid mass with cystic components and internal hemorrhage in a young woman
• Location
Can occur anywhere in pancreas without predisposition for any location
• Size
Average: 5 cm, range: 2.5-20 cm
CT Findings
• Well-defined, heterogeneous, encapsulated mass with thick, enhancing capsule
Usually quite large at presentation (mean > 5 cm)
• Frequent peripheral or central calcification (45-50%)
• Most often solid, but can have variable cystic components and intratumoral hemorrhage
Usually very little enhancement, with “solid” components often representing intratumoral blood products
• Metastatic disease is very uncommon, but most often metastasizes to liver and locoregional lymph nodes
• Usually no biliary or pancreatic ductal obstruction
• Gross vascular invasion or occlusion on imaging is rare
MR Findings
• Large, well-demarcated mass with central areas of low and high T1 signal intensity (hemorrhage)
Presence of internal hemorrhage highly characteristic feature, and may result in fluid-fluid or hematocrit levels
• Solid or cystic with minimal enhancement on T1WI C+
• Capsule appears as rim of low T2 signal intensity and enhances on post-gadolinium images




 in the pancreatic body with a clearly visible enhancing capsule. The mass was found to be a solid pseudopapillary neoplasm (SPEN) at surgery.
in the pancreatic body with a clearly visible enhancing capsule. The mass was found to be a solid pseudopapillary neoplasm (SPEN) at surgery.
 with peripheral rim calcification
with peripheral rim calcification  in the tail of the pancreas. Endoscopic ultrasound (not shown) confirmed a complex cystic mass. Needle aspiration of the mass at ultrasound yielded fluid that had few cells and no elevated tumor markers. The fluid was not mucoid.
in the tail of the pancreas. Endoscopic ultrasound (not shown) confirmed a complex cystic mass. Needle aspiration of the mass at ultrasound yielded fluid that had few cells and no elevated tumor markers. The fluid was not mucoid.
 , compatible with a SPEN.
, compatible with a SPEN.











