and Zdeněk Fryšák1
(1)
Department of Internal Medicine III – Nephrology, Rheumatology and Endocrinology, Faculty of Medicine and Dentistry, Palacky University Olomouc and University Hospital Olomouc, Olomouc, Czech Republic
Keywords
MicrocarcinomaTumor sizeCervical metastatic lymph nodesPapillary thyroid carcinomaSmall noduleTypical US featuresMedium-sized noduleLarge noduleMultifocal papillary thyroid carcinomaHashimoto’s thyroiditisCoexistenceReduce risk of recurrenceGraves’ diseaseAmiodarone-induced thyrotoxicosisParathyroid adenomaCoincidenceFollicular thyroid carcinomaExtrathyroidal extensionTumor thrombusPrognostic factor15.1 Papillary Thyroid Microcarcinoma
15.1.1 Essential Facts
Analysis of the thyroid cancer incidence from 1980 to 2005 (the Surveillance, Epidemiology and End Results/SEER/program of the National Cancer Institute) showed that half of the overall increase in PTC rates is due to rising rates of very small ≤1.0 cm cancers, so-called papillary thyroid microcarcinomas (PTMC) [1].
Prevalence of subclinical PTMC is 1.9–11.7 per 100,000 females; that is about 1000 times higher than that of clinical thyroid carcinoma [2].
PTMC represents 43% of PTC in patients >45 years of age and 34% in patients <45 years of age [3].
The detection rate of PTMC (measuring 3–9.9 mm) in autopsy studies is 0.5–5.2% [2].
Hay et al. at Mayo Clinic investigated 900 patients with PTMC in the period 1945–2004, with a mean follow-up of 17.2 years. Despite tumors being found multifocal in 23%, associated with cervical metastatic lymph nodes (LNs) in 31% and in 0.3% with distant metastases at diagnosis, the 20-year and 40-year tumor recurrence rates were only 6% and 8%, respectively [4].
Currently, post-surgical follow-up of patients with PTMC shows disease-specific mortality rates <1%, cervical metastatic LNs 2–6%, and distant recurrence rates 1–2%. These excellent results are more related to the indolent nature of the disease rather than to the effectiveness of treatment [4, 5].
PTMC mostly showed stable tumor size on average follow-up by US on 5-year follow-up, whereas only 5% showed tumor enlargement (>3 mm) and 8% on 10-year follow-up. Only 1.7% and 3.8% of patients at 5-year and 10-year follow-up showed evidence of LN metastases [2].
Subclinical low-risk PTMCs (no evidence of extrathyroidal extension, cervical metastatic LNs, or distant metastases) often have an indolent course and could be observed without immediate need for surgery. Older patients with subclinical low-risk PTMC may be the best candidates for observation only. PTMC in young patients (<40 years of age) is significantly more progressive, but the cause-specific survival is reported to be excellent. These patients can also be candidates for close US follow-up since it would not be too late for surgery if their subclinical PTMC turned into clinical disease [2].
Meta-analyses revealed that central cervical metastatic LNs (at level C-VI) are associated with male gender, younger age (<45 years), larger tumor size (>5 mm), multifocality, and extrathyroidal extension [6].
When patients with PTMC and PTC were compared, no differences were observed in age, gender, and multifocality. PTMC is associated with less frequent bilaterality, cervical metastatic LNs, thyroid capsule invasion, and disease recurrence, and has a higher rate of incidental diagnosis [7].
15.1.2 US Features of the Papillary Thyroid Microcarcinoma
For PTMC, apply the same 2015 ATA criteria as for other suspected nodules [8].
Typical features of PTMC [9]:
50% of PTMC nodules have a well-defined margin and 50% have an ill-defined margin (and half of those display, on histology, infiltration into the surrounding thyroid tissue (Figs. 15.2aa and 15.4aa).
No cystic changes.
Isoechogenicity (on histology, predominantly follicular structures with large proportion of colloid) (Figs. 15.3aa and 15.4aa).
Heterogeneous echogenicity (on histology, fibrous stroma proportion of >20%) (Fig. 15.4aa)
Cervical metastatic LNs (2–6%) (Fig. 15.4dd).


Fig. 15.1
(aa) A 44-year-old woman with a solitary papillary thyroid microcarcinoma—PTMC (arrowheads) in the LL, size 10 × 8 × 6 mm and volume 0.3 mL: solid; elliptical shape; homogeneous; hypoechoic; one microcalcification (open arrow); well-defined, smooth margin; Tvol 12 mL, RL 6 mL, and LL 6 mL; transverse. (bb) Detail of solitary PTMC (arrowheads), CFDS: peripheral vascularity and one central vessel branch, pattern I; transverse. (cc) Detail of solitary PTMC (arrowheads): hypoechoic; one microcalcification (open arrow); longitudinal. (dd) Detail of solitary PTMC (arrowheads), CFDS: peripheral vascularity and one central vessel branch, pattern I; longitudinal

Fig. 15.2
(aa) A 63-year-old woman with a solitary papillary thyroid microcarcinoma—PTMC (arrowheads) in the RL, size 10 × 9 × 6 mm and volume 0.3 mL: solid; “taller than wide” shape; coarse structure; hypoechoic; cluster of microcalcifications in the center (open arrows); blurred margin; Tvol 8 mL, RL 4 mL and LL 4 mL; transverse. (bb) detail of solitary PTMC (arrowheads): solid; “taller-than-wide” shape; coarse structure; hypoechoic; cluster of microcalcifications in the center (open arrows); blurred margin; transverse. (cc) Detail of solitary PTMC (arrowheads): solid; coarse structure; hypoechoic; cluster of microcalcifications in the center (open arrows); blurred; longitudinal

Fig. 15.3
(aa) A 62-year-old woman with a solitary papillary thyroid microcarcinoma—PTMC (arrowheads) in the LL, size 8 × 7 × 6 mm and volume 0.2 mL: solid; round shape; inhomogeneous structure; isoechoic; sporadically hyperechoic punctuation (open arrows); thin halo sign; Tvol 8 mL, RL 4 mL, and LL 4 mL; transverse. (bb) Detail of solitary PTMC (arrowheads): inhomogeneous structure; isoechoic; sporadically hyperechoic punctuation (open arrows); well-defined margin with thin halo sign; transverse. (cc) Detail of solitary PTMC (arrowheads): inhomogeneous; isoechoic; sporadically hyperechoic punctuation (open arrows); well-defined margin with thin halo sign; longitudinal


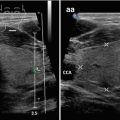
Fig. 15.4
(aa) A 30-year-old woman with a solitary, papillary thyroid microcarcinoma (PTMC) in the RL, size 10 × 9 × 8 mm, volume 0.4 mL and small metastatic cervical lymph nodes (LNs) along right IJV, at level C-III. Overall view of thyroid gland: PTMC (arrowheads)—solid; “taller-than-wide” shape; inhomogeneous structure; isoechoic; central hyperechoic punctuation (open arrows); ill-defined margin with thick halo sign; Tvol 14 mL, RL 7 mL, and LL 7 mL; transverse. (bb) Detail of solitary PTMC (arrowheads): inhomogeneous structure; isoechoic; central hyperechoic punctuation (open arrows); ill-defined margin with thick halo sign; longitudinal. (cc) Detail of solitary PTMC and metastatic cervical LNs: PTMC (arrowheads)—“taller-than-wide” shape; inhomogeneous structure; isoechoic; central hyperechoic punctuation (open arrows); one small oval hyperechoic metastatic ln1 (marks) between the right IJV and CCA; transverse. (dd) Detail of two metastatic cervical LNs: ln1, ln2 (marks)—solid; elliptical shape; size 19 × 7 mm and 16 × 6 mm, L/S ratio > 2 (not pathological); inhomogeneous structure; hyperechoic; no hilus sign; lumen of small vein (v) between LNs; longitudinal. (ee) Detail of two metastatic cervical LNs, CFDS: ln1, ln2 (marks)—increased mixed (peripheral and central) vascularity; lumen of small vein (v) between LNs; longitudinal
15.2 Papillary Thyroid Carcinoma: A Small Solitary Nodule ≤2 cm
15.2.1 Essential Facts
The most common histological type of thyroid cancer among all sex and racial/ethnic groups is papillary thyroid carcinoma (PTC), range: 65–88% [1].
PTC rate is consistently two to three times higher among females than males. The highest rates occurred among females aged 40–59, but the steepest increases were observed among those aged 60–79. Age-specific rates among men rise more slowly, peaking at ages 60–69 years for both genders; then decline at ages ≥80 years [1, 10].
The youngest (<20 years) and oldest (≥80 years) age groups each accounts for only 2–3% of the PTC [1].
Features predicting a poor prognosis of PTC patients: old age, extrathyroidal and/or extranodal extension, palpable lymph node (LN) and/or distant metastases, and large tumor size [11].
Tg-Ab positive patients with no postoperative decrease in the Tg-Ab level have a poor prognosis of disease-free survival [12].
PTC prognosis is excellent, reflecting a 5- and 10-year survival rate of 90–95% [13].
Recurrence of PTC develops in about 20% of patients [14].
PTC tends to metastasize through the lymphatic system, with cervical metastatic LNs occurring in 40–60%, and vascular invasion occurs in 2–14% [13].
The vascular invasion was found in 3.3% of pure PTC, compared with 20.9% of cases of the follicular variant of papillary carcinoma (FVPTC) [13].
The incidence of PTC is growing at a faster rate than any other malignancy. Nearly 50% of the increase proved to be PTC of 1 cm or smaller, and 87% were ≤2 cm. However, thyroid cancer mortality has remained flat, implying that these small cancers would not likely have progressed to be life-threatening. This dramatic rise in subclinical disease has been attributed largely to more frequent and widespread use of imaging of the head and neck for unrelated investigations, with the unanticipated discovery of these incidental cancers [15].
Comparison PTC vs. FTC (both differentiated thyroid carcinomas) [16]:
Higher incidence 3.9:1.
Manifestation in a younger age, median age, 44 vs. 49.
Higher female-male ratio, 4.5 vs. 2.9.
Smaller primary tumor size, median 2 cm vs. 3.5 cm.
Higher incidence of multifocal disease, 28.3% vs. 18.1%.
Frequent extrathyroidal extension, 39.4% vs. 14%.
More cervical metastatic LNs, 33.3% vs. 12.1%.
Less distant metastases 8.9% vs. 28.8%.
The 10-year cause-specific survival, freedom from distant metastasis, and locoregional failure figures for PTC compared with FTC were 92.1% vs. 81%, 90.8% vs. 72.3%, and 78.5% vs. 83%.
15.2.2 US Features of PTC, a Small Nodule ≤2 cm [8]
Typical US features:


Fig. 15.5
(aa) A 43-year-old woman with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 15 × 14 × 14 mm and volume 1.5 mL. US overall view: solid nodule—round shape; homogeneous structure; hypoechoic; well-defined margin; Tvol 18 mL, RL 10 mL, and LL 8 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—round shape; homogeneous structure; hypoechoic; well-defined margin; transverse. (cc) Detail of solitary small PTC (arrowheads), CFDS: minimal peripheral vascularity and one central vessel branch, pattern I; transverse. (dd) Detail of solitary small PTC (arrowheads): solid nodule—round shape; homogeneous structure; hypoechoic; well-defined margin; longitudinal. (ee) Detail of solitary small PTC (arrowheads), CFDS: minimal peripheral vascularity and one central vessel branch, pattern I; longitudinal

Fig. 15.6
(aa) A 37-year-old woman with multinodular goiter (MNG) and a small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 13 × 12 × 12 mm and volume 1 mL. US overall view: solid nodule—round shape; homogeneous structure; hypoechoic; well-defined margin; Tvol 10 mL, RL 6 mL, and LL 4 mL; transverse. (bb) Detail of small PTC (arrowheads), CFDS: minimal peripheral and intranodular vascularity, pattern I; transverse. (cc) Detail of small PTC (arrowheads) in MNG, RL: PTC—solid nodule; round shape; homogeneous structure; hypoechoic; well-defined margin; three nonsuspicious nodules (1, 2, 3)—solid; round or ovoid shape; homogeneous structure; hyperechoic; well-defined margin with halo sign; longitudinal


Fig. 15.7
(aa) A 44-year-old man with a solitary small papillary thyroid carcinoma—PTC (arrowheads), size 19 × 14 × 11 mm and volume 1.5 mL in the LL. US overall view: solid nodule—“taller-than-wide” shape; inhomogeneous structure; slightly hypoechoic; diffusely hyperechoic punctuation; blurred margin; Tvol 20 mL, RL 10 mL, and LL 10 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—“taller-than-wide” shape; inhomogeneous structure; slightly hypoechoic; diffusely hyperechoic punctuation; blurred margin; transverse. (cc) Detail of solitary small PTC (arrowheads): solid nodule—“taller-than-wide” shape; inhomogeneous structure; slightly hypoechoic; diffusely hyperechoic punctuation; blurred margin; longitudinal. (dd) Detail of solitary small PTC (arrowheads), CFDS: minimal peripheral vascularity, pattern I; longitudinal


Fig. 15.8
(aa) A 48-year-old man with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the LL, size 19 × 14 × 11 mm and volume 1.5 mL. US overall view: solid nodule—“taller-than-wide” shape; inhomogeneous structure; hypoechoic; central microcalcifications (arrow); microlobulated margin; Tvol 22 mL, RL 11 mL, and LL 11 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—“taller-than-wide” shape; inhomogeneous structure; hypoechoic; central microcalcifications (arrow); microlobulated margin; transverse. (cc) Detail of solitary small PTC (arrowheads): solid nodule—“taller-than-wide” shape; inhomogeneous structure; hypoechoic; central microcalcifications (arrow); microlobulated margin; longitudinal. (dd) Detail of solitary small PTC (arrowheads), CFDS: minimal peripheral vascularity, pattern I; longitudinal

Fig. 15.9
(aa) A 38-year-old man with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 17 × 14 × 7 mm and volume 1 mL. US overall view: solid nodule—oval shape; inhomogeneous structure; slightly hypoechoic; diffusely hyperechoic punctuation; peripheral arc of microcalcifications (arrows); blurred margin; Tvol 22 mL, RL 7 mL, and LL 5 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—oval shape; inhomogeneous structure; slightly hypoechoic; diffusely hyperechoic punctuation; peripheral arc of microcalcifications (arrows); blurred margin; transverse. (cc) Detail of solitary small PTC (arrowheads): solid nodule—oval shape; inhomogeneous structure; slightly hypoechoic; diffuse hyperechoic punctuation; peripheral circular rim of microcalcifications (arrows); blurred margin; longitudinal
Rare US features:

Fig. 15.10
(aa) A 55-year-old man with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 15 × 11 × 11 mm and volume 1 mL. US overall view: interrupted rim peripheral “eggshell” calcification (arrows) with prominent acoustic shadow causing hypoechogenicity of intranodular structure; Tvol 15 mL, RL 7 mL, and LL 8 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): interrupted rim peripheral “eggshell” calcification (arrows) with prominent acoustic shadow causing hypoechogenicity of intranodular structure; transverse. (cc) Detail of solitary small PTC (arrowheads): interrupted rim peripheral “eggshell” calcification (arrows) with prominent acoustic shadow causing hypoechogenicity of intranodular structure; longitudinal


Fig. 15.11
(aa) A 43-year-old woman with a small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 12 × 12 × 11 mm and volume 1 mL. US overall view: solid nodule—round shape; homogeneous structure; mostly isoechoic; centrally tiny hypoechoic area; well-defined margin; irregular thick halo sign; tiny hypoechoic nodule in the LL; Tvol 13 mL, RL 7 mL, and LL 6 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—round shape; homogeneous structure; mostly isoechoic; centrally tiny hypoechoic area; well-defined margin; irregular thick halo sign; transverse. (cc) Detail of small PTC (arrowheads), CFDS: avascular node, pattern 0; transverse. (dd) Detail of solitary small PTC (arrowheads): solid nodule—round shape; homogeneous structure; mostly isoechoic; centrally tiny hypoechoic area; well-defined margin; irregular thick halo sign; longitudinal


Fig. 15.12
(aa) A 44-year-old man with a solitary small papillary thyroid carcinoma, follicular variant—FVPTC (arrowheads) in the RL, size 13 × 12 × 12 mm and volume 1 mL. US overall view: solid nodule—round shape; inhomogeneous structure; isoechoic; diffusely hyperechoic punctuation; centrally tiny hypoechoic area; blurred margin; Tvol 8 mL, RL 5 mL, and LL 3 mL; transverse. (bb) Detail of solitary small FVPTC (arrowheads): solid nodule—round shape; inhomogeneous structure; isoechoic; diffusely hyperechoic punctuation; centrally tiny hypoechoic area; blurred margin; transverse. (cc) Detail of small FVPTC (arrowheads), CFDS: focally increased peripheral and intranodular vascularity, pattern II; transverse. (dd) Detail of solitary small FVPTC (arrowheads): solid nodule—round shape; inhomogeneous structure; isoechoic; diffusely hyperechoic punctuation; centrally tiny hypoechoic area; blurred margin; longitudinal. (ee) Detail of small FVPTC (arrowheads), CFDS: peripheral vascularity, pattern I; transverse.


Fig. 15.13
(aa) A 56-year-old woman with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 19 × 14 × 11 mm and volume 1.5 mL. US overall view: solid nodule—ovoid shape; homogeneous structure; mostly isoechoic; small round hypoechoic area at periphery “nodule in a nodule” appearance; well-defined margin; thin halo sign around isoechoic part; Tvol 13 mL, RL 7 mL, and LL 6 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): solid nodule—ovoid shape; homogeneous structure; mostly isoechoic; small round hypoechoic area (open arrows): at periphery like “nodule in a nodule” appearance; well-defined margin; thin halo sign around isoechoic part; transverse. (cc) Detail of small PTC (arrowheads), CFDS: increased peripheral vascularity and markedly in intranodular hypoechoic “nodule” (open arrows), pattern II; transverse. (dd) Detail of solitary small PTC (arrowheads): solid nodule—ovoid shape; homogeneous structure; mostly isoechoic; small round hypoechoic area (open arrows) at periphery “nodule in a nodule” appearance; well-defined margin; thin halo sign around isoechoic part; longitudinal. (ee) Detail of small PTC (arrowheads), CFDS: increased peripheral vascularity and markedly in intranodular hypoechoic “nodule” (open arrows), pattern II; longitudinal


Fig. 15.14
(aa) A 34-year-old woman with a solitary small papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 23 × 15 × 11 mm and volume 2 mL. US overall view: complex, predominantly solid nodule—ovoid shape; solid part inhomogeneous structure; mostly hyperechoic; central coarse linear calcification (arrow) with acoustic shadow; suspicious small hypoechoic part (open arrows) above calcification; small cystic cavity (c) at periphery; blurred margin; Tvol 13 mL, RL 7 mL, and LL 6 mL; transverse. (bb) Detail of solitary small PTC (arrowheads): complex, predominantly solid nodule—ovoid shape; solid part inhomogeneous structure; mostly hyperechoic; central coarse linear calcification (arrow) with acoustic shadow; suspicious small hypoechoic part above calcification; small cystic cavity (c) at periphery; blurred margin; transverse. (cc) Detail of small PTC (arrowheads), CFDS: sporadic peripheral vascularity and markedly increased intranodular vascularity in hypoechoic part (open arrows), pattern II; transverse. (dd) Detail of solitary small PTC (arrowheads): complex, predominantly solid nodule—ovoid shape; solid part inhomogeneous structure; mostly hyperechoic; central coarse linear calcification (arrow) with acoustic shadow; suspicious small hypoechoic part (open arrows) above calcification; blurred margin; longitudinal. (ee) Detail of small PTC (arrowheads), CFDS: sporadic peripheral vascularity and markedly increased intranodular vascularity in hypoechoic part (open arrows), pattern II; longitudinal


Fig. 15.15
(aa) A 30-year-old man with a solitary medium-sized papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 27 × 25 × 16 mm and volume 5 mL. Moreover small metastatic cervical lymph nodes (LN) along the right IJV at level C-III, IV. US overall view: solid nodule—irregular shape, inhomogeneous structure; isoechoic or slightly hypoechoic; foci of microcalcifications (open arrows); lobulated blurred margin; Tvol 18 mL, asymmetry—RL 12 mL and LL 6 mL; transverse. (bb) Detail of solitary medium-sized PTC (arrowheads): solid nodule—irregular shape, inhomogeneous structure; isoechoic or slightly hypoechoic; foci of microcalcifications (open arrows); lobulated blurred margin; transverse. (cc) Detail of solitary medium-sized PTC (arrowheads), CFDS: increased peripheral and intranodular vascularity, pattern II; transverse. (dd) Detail of solitary medium-sized PTC (arrowheads): solid nodule—inhomogeneous structure; isoechoic or slightly hypoechoic; foci of microcalcifications (open arrows); lobulated blurred margin; longitudinal. (ee) Detail of solitary medium-sized PTC (arrowheads) and one tiny metastatic LN at level C-III: ln1—round shape, size 5 mm; homogeneous structure; hyperechoic; no hilus sign; transverse. (ff) Detail of three small metastatic LN at level C-III, IV: ln1—oval shape, size 9 × 5 mm; ln2—elliptical shape, size 15 × 4 mm and ln3—size 11 × 3 mm, L/S ratio ≈ 2 (not pathological); homogeneous structure; hyperechoic; no hilus sign; longitudinal


Fig. 15.16
(aa) A 42-year-old woman with multinodular goiter and medium-sized papillary thyroid carcinoma—PTC in the LL, size 28 × 20 × 18 mm and volume 5 mL. Moreover small metastatic cervical lymph nodes (LN) along the left IJV at level C-II, III. Personal history: 20 years post radiotherapy for Hodgkin’s lymphoma. US overall view: suspicious solid nodule (arrowheads) in the LL—round shape; inhomogeneous structure; mixed echogenicity with irregular hypoechoic areas; linear calcifications at periphery (arrows); microlobulated margin; nonsuspicious complex nodule in the RL—hyperechoic; central septated cystic cavity (c); well-defined margin with thin halo sign; Tvol 18 mL, asymmetry—RL 12 mL and LL 6 mL; transverse. (bb) Detail of medium-sized PTC (arrowheads) in the LL: solid nodule—suspicious solid nodule (arrowheads) in the LL—round shape; inhomogeneous structure; mixed echogenicity with irregular hypoechoic areas; linear calcifications at periphery (arrows); microlobulated margin; transverse. (cc) Detail of medium-sized PTC (arrowheads) in the LL, CFDS: increased peripheral and sporadic intranodular vascularity, pattern II; transverse. (dd) Detail of medium-sized PTC (arrowheads) and one metastatic LN1 (blank arrowheads) at level C-III: LN1—elliptical shape, size 16 × 10 mm; inhomogeneous structure; solid part hyperechoic; central hyperechoic punctuation; sporadic cystic (c) necrosis; no hilus sign; transverse. (ee) Detail of metastatic LN1 (blank arrowheads) at level C-III: elliptical shape, size 23 × 10 mm, L/S ratio ≈ 2 (not pathological); inhomogeneous structure; solid part hyperechoic; central hyperechoic punctuation; sporadic cystic (c) necrosis; no hilus sign; longitudinal. (ff) Detail of two tiny metastatic LN at level C-II: ln2—oval shape, size ≈ 10 mm and ln3—size ≈ 6 mm; homogeneous structure; hyperechoic; no hilus sign; transverse


Fig. 15.17
(aa) A 27-year-old woman with a solitary medium-sized papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 34 × 21 × 20 mm and volume 7.5 mL. Moreover small metastatic cervical lymph nodes (LN) along the right IJV at level C-II, III. US overall view: solid nodule—oval shape, inhomogeneous structure; hyperechoic; diffusely hyperechoic punctuations (open arrows); well-defined margin; incomplete thin halo sign; Tvol 15 mL, asymmetry—RL 10 mL and LL 5 mL; transverse. (bb) Detail of solitary medium-sized PTC (arrowheads): solid nodule—oval shape, inhomogeneous structure; hyperechoic; diffusely hyperechoic punctuations (open arrows); well-defined margin; incomplete thin halo sign; longitudinal. (cc) Detail of solitary medium-sized PTC (arrowheads), CFDS: sporadic peripheral and intranodular vascularity, pattern I; longitudinal. (dd) Detail of a lone metastatic LN at level C-II: LN1—elliptical shape, size 18 × 9 mm; inhomogeneous structure; slightly hyperechoic; no hilus sign; transverse. (ee) Detail of solitary medium-sized PTC (arrowheads) and another small metastatic LN at level C-III: LN3—oval shape, size 14 × 9 mm; homogeneous structure; hyperechoic; no hilus sign; transverse. (ff) Detail of three small metastatic LN at level C-III: tiny ln2—elliptical shape, size 7 × 3 mm; small LN3—elliptical shape, size 25 × 9 mm, L/S ratio ≈ 2 (not pathological); and tiny ln4, size 5 mm; all LNs—homogeneous structure; hyperechoic; no hilus sign; longitudinal


Fig. 15.18
(aa) An 80-year-old woman with a solitary medium-sized papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 34 × 32 × 14 mm and volume 8 mL. Moreover metastatic cervical lymph nodes (LN) along the right CCA at level C-II, III. US overall view: complex nodule—elliptical shape, “more wide than tall”; coarse structure; mixed echogenicity, solid part mostly hyperechoic with multiple microcalcifications (open arrows), small irregular cystic cavities (c); microlobulated margin; incomplete thin halo sign; Tvol 33 mL, asymmetry—RL 29 mL and LL 8 mL; transverse; depth of penetration 4 cm. (bb) Detail of medium-sized PTC (arrowheads): complex nodule—coarse structure; solid part mostly hyperechoic with coarse linear calcifications (line of open arrows) and multiple microcalcifications (open arrows) with acoustic shadow, small irregular cystic cavities (c); microlobulated margin; incomplete thin halo sign; transverse. (cc) Detail of medium-sized PTC (arrowheads), CFDS: increased vascularity, pattern II; transverse. (dd) Detail of medium-sized PTC (arrowheads): complex nodule—coarse structure; solid part mostly hyperechoic with coarse curvilinear calcifications (line of open arrows) with acoustic shadow and single microcalcification (open arrow), small irregular cystic cavities (c); microlobulated margin; incomplete thin halo sign; longitudinal. (ee) Detail of medium-sized PTC and solid metastatic LN along the right CCA at level C-III: complex nodule—coarse structure; multiple microcalcifications (open arrows), small cystic cavities (c) hypoechoic periphery; ln 1—oval shape; size 12 × 8 mm; coarse structure; hyperechoic; multiple microcalcifications (open arrows); no hilus sign; transverse. (ff) Detail of two large metastatic LN with cystic necrosis along the right CCA at level C-II: LN2—size 36 × 18 mm and LN3—size 17 × 11 mm, L/S ratio ≈ 2 (not pathological); completely anechoic contents with sporadic septa; no hilus sign; transverse


Fig. 15.19
(aa) A 61-year-old woman with a medium-sized papillary thyroid carcinoma—PTC (arrowheads) in the RL, size 35 × 23 × 21 mm and volume 9 mL. No metastatic cervical lymph nodes. US overall view: solid nodule—inhomogeneous structure; mixed echogenicity, central mostly hyperechoic and markedly hypoechoic periphery; well-defined margin; Tvol 26 mL, asymmetry—RL 19 mL and LL 7 mL; transverse. (bb) Detail of medium-sized PTC (arrowheads): solid nodule—inhomogeneous structure; central mostly hyperechoic and markedly hypoechoic periphery; well-defined margin; transverse. (cc) Detail of medium-sized PTC (arrowheads), CFDS: sporadic peripheral and central vascularity, pattern I; transverse. (dd) Detail of medium-sized PTC (arrowheads): solid nodule—inhomogeneous structure; central mostly hyperechoic and markedly hypoechoic periphery; well-defined margin; “daughter” small nodule (arrows), size 11 × 7 mm with the same pattern next to the upper pole of PTC; longitudinal


Fig. 15.20
(aa) A 33-year-old man with a solitary medium-sized papillary thyroid carcinoma, follicular variant—FVPTC (arrowheads) in the RL, size 34 × 33 × 27 mm and volume 15 mL. Moreover tiny metastatic cervical lymph nodes (LN) along the right IJV at level C-III. US overall view: solid nodule; round shape; coarse structure; mixed echogenicity, central hyperechoic with multiple microcalcifications (open arrows), hypoechoic periphery; ill-defined, lobulated margin; Tvol 33 mL, asymmetry—RL 29 mL and LL 8 mL; transverse; depth of penetration 4 cm. (bb) Detail of medium-sized FVPTC (arrowheads): solid nodule; round shape; coarse structure; mixed echogenicity, central hyperechoic with multiple microcalcifications (open arrows), laterally with acoustic shadow, hypoechoic periphery; ill-defined, lobulated margin; transverse. (cc) Detail of medium-sized FVPTC (arrowheads): solid nodule; round shape; coarse structure; mixed echogenicity, central hyperechoic with multiple microcalcifications (open arrows) with acoustic shadow, hypoechoic periphery; ill-defined, lobulated margin; longitudinal. (dd) Detail of medium-sized FVPTC (arrowheads), CFDS: minimal vascularity, pattern 0; longitudinal. (ee) Detail of medium-sized FVPTC and tiny metastatic LNs: ln1—round shape; size 7 × 5 mm, long-to-short axis ratio ≈ 1; hyperechoic; no hilus sign; transverse. (ff) Detail of medium-sized FVPTC and tiny metastatic LNs: ln2—elliptical shape; size 10 × 5 mm, L/S ratio ≈ 2 (not pathological); hyperechoic; no hilus sign; transverse.



Fig. 15.21
(aa) A 52-year-old woman with a solitary giant papillary thyroid carcinoma—PTC (arrowheads) consist of entire RL, size 60 × 47 × 38 mm and volume 56 mL. Moreover metastatic cervical lymph nodes (LN) along the right CCA at level C-II, III, IV. US overall view: complex nodule—irregular shape; coarse structure; solid part hyperechoic with multiple coarse calcifications (arrows) with acoustic shadow, large irregular cystic cavities (C); ill-defined, lobulated margin; normal structure of LL; trachea and LL push to the left; Tvol 33 mL, asymmetry—RL 56 mL and LL 9 mL; transverse; depth of penetration 6 cm. (bb) Detail of giant PTC (arrowheads): complex nodule—irregular shape; coarse structure; solid part hyperechoic with multiple coarse calcifications (arrows), multiple irregular cystic cavities (c); ill-defined, lobulated margin; transverse. (cc) Detail of giant PTC (arrowheads), another view: complex nodule—irregular shape; coarse structure; solid part hyperechoic with microcalcifications (open arrows), large cystic cavities (C); ill-defined, lobulated or blurred margin; transverse. (dd) Detail of giant PTC (arrowheads): complex nodule—irregular shape; coarse structure; solid part hyperechoic with multiple coarse calcifications (arrows) with acoustic shadow, multiple irregular cystic cavities (C); ill-defined, lobulated or blurred margin; longitudinal. (ee) Detail of giant PTC and large solid metastatic LN size 43 × 25 × 15 mm and volume 8 mL along the right IJV and CCA at level C-II: lateral part of PTC (arrowheads); LN 1—elliptical shape; homogeneous structure; hyperechoic; no hilus sign; compressing IJV; transverse. (ff) Detail of giant PTC and medium-sized complex metastatic LN with cystic necrosis, size 26 × 22 × 16 mm and volume 4.5 mL along the right IJV and CCA at level C-III: lateral part of PTC (arrowheads) with cystic cavity (C); LN2—elliptical shape; inhomogeneous structure; solid part hyperechoic; microcalcifications (open arrows); irregular cystic cavity (c); no hilus sign; transverse. (gg) Detail of giant PTC and large complex metastatic LN with cystic and coagulation necrosis (arrows), size 37 × 35 × 23 mm and volume 16 mL along the right CCA at level C-IV: lateral part of PTC (arrowheads) with cystic cavity (c); LN3—elliptical shape; inhomogeneous structure; hypoechoic with debris and coarse hyperechoic foci without acoustic shadow (arrows); no hilus sign; transverse. (hh) Detail of medium-sized complex metastatic LN2 with cystic necrosis at level C-III and large complex metastatic LN3 with cystic and coagulation necrosis (arrows) at level C-IV: LN2—microcalcifications (open arrows); irregular cystic cavity (c); LN3—hypoechoic with debris and coarse hyperechoic foci without acoustic shadow (arrows); longitudinal. (ii) Detail of medium-sized complex metastatic LN2 with cystic necrosis at level C-III and large complex metastatic LN3 with cystic and coagulation necrosis at level C-IV, CFDS: both LNs hilar vascularity; longitudinal


Fig. 15.22
(aa) A 37-year-old man with a multifocal papillary thyroid carcinoma (PTC)—papillary thyroid microcarcinoma (PTMC) in the RL and small papillary thyroid carcinoma (PTC) in the isthmus and three cervical metastatic lymph nodes (LN) bilaterally. US scan of PTMC (arrowheads), size 12 × 9 × 8 mm and volume 0.4 mL in the RL: solid nodule; “taller-than-wide” shape; inhomogeneous structure; hypoechoic; centrally microcalcifications (open arrows); ill-defined blurred margin; Tvol 21 mL, RL 11 mL, and LL 10 mL; transverse. (bb) Detail of PTMC in the RL and metastatic LN along the right CCA at level C-VI: PTMC (arrowheads)—solid nodule; “taller-than-wide” shape; inhomogeneous structure; hypoechoic; centrally microcalcifications (open arrows); ill-defined blurred margin; metastatic LN1 (marks)—round shape; size 15 × 12 mm, L/S ratio ≈ 1; homogeneous structure; hypoechoic; no hilus sign; longitudinal. (cc) Detail of small PTC size 15 × 12 × 9 mm, volume 0.8 mL in low side of isthmus and metastatic LN in the low neck at level C-VI: PTC (arrowheads)—solid nodule; round shape; coarse structure; mostly hypoechoic; peripheral microcalcifications (open arrows); ill-defined blurred margin; metastatic LN2 (marks)—round shape; homogeneous structure; hypoechoic; hyperechoic band, no hilus sign; transverse. (dd) Detail of PTC in low side of isthmus and metastatic LN on the low neck at level C-VI: PTC (arrowheads)—solid nodule; ovoid shape; coarse structure; mostly hypoechoic; peripheral microcalcifications (open arrows); ill-defined blurred margin; metastatic LN2 (marks)—round shape, size 14 × 13 mm, L/S ratio ≈ 1; homogeneous structure; hypoechoic; no hilus sign; longitudinal. (ee) Detail of two metastatic LNs under low poles bilaterally at level C-VI: metastatic LN1, LN2 (marks)—round shape, L/S ratio ≈ 1; homogeneous structure; hypoechoic; no hilus sign; transverse. (ff) Detail of two metastatic LNs under low pole of the LL at level C-VI: metastatic LN2 (marks) size 14 × 13 mm, LN3 (marks) size 16 × 16 mm—round shape, L/S ratio ≈ 1; homogeneous structure; hypoechoic; no hilus sign; longitudinal


Fig. 15.23
(aa) A 48-year-old woman with a multifocal papillary thyroid carcinoma (PTC)—papillary thyroid microcarcinoma (PTMC) size 8 × 7 × 6 mm, volume 0.2 mL in the RL and medium-sized papillary thyroid carcinoma (PTC) size 18 × 15 × 14 mm, volume 2 mL in the LL; without cervical metastatic lymph nodes. US overall view: PTMC (arrows)—solid nodule; round shape; inhomogeneous structure; mixed echogenicity; sporadic microcalcifications (open arrows); well-defined margin; thin halo sign; PTC (arrowheads)—solid nodule; “taller-than-wide” shape; coarse structure; mixed echogenicity; diffusely microcalcifications (open arrows); ill-defined blurred margin; Tvol 15 mL, RL 7 mL, and LL 8 mL; transverse. (bb) Detail of medium-sized PTC (arrowheads) in the LL: solid nodule; “taller-than-wide” shape; coarse structure; mixed echogenicity; diffusely microcalcifications (open arrows); ill-defined blurred margin; transverse. (cc) Overall view of PTMC and PTC, CFDS: PTMC (arrows)—avascular, pattern 0; PTC (arrowheads)—sporadic peripheral and parenchymal vascularity, pattern I; transverse. (dd) Detail of PTMC (arrows) in the RL: solid nodule; round shape; inhomogeneous structure; mixed echogenicity; centrally sporadic microcalcifications (open arrows); well-defined margin; thin halo sign; longitudinal. (ee) Detail of PTC (arrowheads) in the LL: solid nodule; round shape; coarse structure; mixed echogenicity; diffusely microcalcifications (open arrows); ill-defined blurred margin; longitudinal. (ff) Detail of PTC in the LL, CFDS: sporadic peripheral and parenchymal vascularity, pattern I; longitudinal


Fig. 15.24
(aa) A 33-year-old man with a multifocal papillary thyroid carcinoma (PTC)—dominant large PTC, size 31 × 24 × 23 mm, volume 9 mL in the LL and two small PTCs in the RL and LL sized ≈ 10 mm. Moreover cervical metastatic lymph nodes (LN) along the left IJV at level C-IV. US overall view: large PTC (arrowheads) in the LL dorsally—solid nodule; “taller-than-wide” shape; coarse structure; hypoechoic; diffusely microcalcifications (open arrows); ill-defined blurred margin; small PTC (arrows) in the LL ventrally—solid nodule; round shape; homogeneous structure; isoechoic; sporadic microcalcifications (open arrows) at periphery; ill-defined margin; small PTC (arrows) in the RL—solid nodule; round shape; inhomogeneous structure; hypoechoic; centrally microcalcifications (open arrows); ill-defined slurred margin; Tvol 31 mL, RL 11 mL, and LL 20 mL; transverse. (bb) Detail of large PTC (arrowheads) in LL: solid nodule; “taller-than-wide” shape; coarse structure; hypoechoic; diffusely microcalcifications (open arrows); ill-defined blurred margin; tumor protrusion ventrally with contour bulging and interrupting continuity of the capsule (arrows); transverse. (cc) Detail of large PTC (arrowheads) in LL, CFDS: sporadic peripheral vascularity, pattern I; transverse. (dd) Detail of large PTC (arrowheads) in LL: solid nodule; “taller-than-wide” shape; coarse structure; hypoechoic; diffusely microcalcifications (open arrows); ill-defined blurred margin; tumor protrusion ventrally with contour bulging and interrupting continuity of the capsule (arrows); longitudinal. (ee) Detail of large PTC (arrowheads) in LL and two tiny metastatic LNs along the left IJV at level C-IV: ln1 (marks)—elliptical shape, size 9 × 4 mm, L/S ratio > 2 (not pathological); homogeneous structure; hyperechoic; no hilus sign; transverse. (ff) Detail of large PTC (arrowheads) in LL and two tiny metastatic LNs along the left IJV at level C-IV: ln2 (marks)—elliptical shape, size 10 × 4 mm, L/S ratio > 2 (not pathological); homogeneous structure; hyperechoic; no hilus sign; transverseRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree