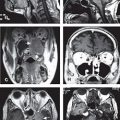
New Target Delineation Contours
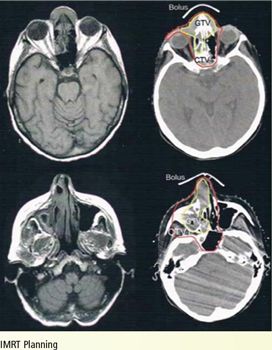
FIGURE 5-7. CTV1 and CTV2 delineation in a patient with clinically T4N2bM0 squamous cell carcinoma of the nasal cavity who received definitive IMRT. The patient presented with a nasal mass. CT showed a tumoral lesion originating from the nasal cavity, extending into the orbital cavity and maxillary sinus. Both the primary site and the bilateral neck were treated with definitive IMRT.
1. ANATOMY
1.1. Nasal Cavity
• The nasal cavity begins at the limen nasi and extends posteriorly to the choana. The choanae communicate directly with the nasopharynx. The nasal cavity is located between the base of the cranium superiorly and the hard palate inferiorly. It is divided into right and left halves by a midline septum. The bones and cartilages that compose the roof and sides of the external nose are shown in Figures 5-1 and 5-2.
• The vomer articulates with the body of sphenoid and makes the posteroinferior portion of the septum. The perpendicular plate of the ethmoid makes up the superior aspect of the septum and is contiguous with the cribriform plate, which is paper-thin and offers minimal protection to tumor invasion. The septum is frequently deviated to one side of the nasal cavity.
• There are three turbinates (inferior, middle, and superior), or conchae, which are projections from the lateral wall of the nasal cavity and act to warm, humidify, and filter air. The spaces between the inferior turbinate and floor of the nasal cavity, between the middle and inferior turbinates, and between the superior and middle turbinates are the inferior, middle, and superior meatus, respectively (Fig. 5-3). The nasolacrimal duct enters the nasal cavity through the inferior meatus. The frontal sinus and anterior ethmoid cells communicate with the nasal cavity through the middle meatus. The posterior ethmoid cells and sphenoid sinuses open into the superior meatus.
• The pterygopalatine fossa is situated inferiorly to the inferior orbital fissure, and the infraorbital nerve is located superior to this fossa as it enters the foramen rotundum.
1.2. Ethmoid Sinus
• The ethmoid sinus is composed of numerous air cells, which are located between the medial walls of the orbit and the lateral walls of the nasal cavity (Fig. 5-3). These air cells are divided into two main groups: anterior and posterior ethmoid cells. The partition between these cavities is thin and gives no resistance to tumor spread.
• The ethmoid sinus is bordered laterally by the lacrimal bone and the lamina papyracea. The lamina papyracea is the lateral plate of the ethmoid labyrinth bone, which forms a large part of the medial orbital wall. Due to its thin and extremely porous nature, the lamina papyracea offers little resistance to tumor spread into the orbit from the ethmoid sinus. The roof of the ethmoid sinuses is the skull base. The fovea ethmoidalis is the thin orbital plate of the frontal bone that comprises the roof of the ethmoid cells. The posterior ethmoid cells are closely related to the optic canal and optic nerve.
• The olfactory nerve is a collection of sensory nerve fibers that extend from the nasal cavity up to the olfactory bulbs, which lie on the ventral aspect of the frontal lobes, through the perforations within the cribriform plate of the ethmoid bone. As the fibers of the olfactory nerve penetrate the cribriform plate, it provides a route for tumor invasion into the anterior cranial fossa.
1.3. Sphenoid Sinus
• The sphenoid sinus is the most posterior paranasal sinus and is contained in the body of the sphenoid bone. The hypophysis and optic chiasm are located superiorly, the cavernous sinuses and carotid arteries are located laterally, the nasal cavity and ethmoid sinuses are located anteriorly, and the nasopharynx is located inferiorly. The clivus and brainstem are situated posteriorly. Each sphenoid sinus communicates with the nasal cavity via the sphenoethmoid recess, by means of an aperture in the anterior wall of the sinus.
• The right and left sphenoid sinuses are divided by a septum. Because the septum is often incomplete or, at best, very thin, it is rarely located in the anatomic midline, and the sphenoid sinuses are often asymmetric.
1.4. Maxillary Sinus
• Each maxillary sinus forms a pyramidal structure: it is bordered medially by the nasal cavity, superiorly by the floor of the orbit, anterolaterally by the facial bone, and posteromedially by the infratemporal fossa. The nasal wall forms the base, and the apex extends into the zygomatic process of the maxilla. Behind the posterior wall of the maxillary sinus lies the pterygomaxillary fossa, which contains the internal maxillary artery, sphenopalatine ganglion, vidian canal, greater palatine nerve, and foramen rotundum.
• The roots of the first and second molar teeth, and occasionally of other teeth, project into the floor of the sinus. The level of the floor varies during the course of a lifetime as the maxillary sinus pneumatizes. Typically from birth into adolescence the floor of the sinus is above that of the nasal cavity; the floor gradually sinks during pneumatization so that by mid-adolescence and adulthood, when the maxillary sinus is fully developed, the floor moves below the floor of the nasal cavity.
1.5. Frontal Sinus
• The frontal sinuses are contained between the lamina of the frontal bones and are rarely symmetric as they are separated by a bony septum that frequently deviates from the midline. The posterior wall of frontal sinuses, which separates them from the anterior cranial fossa, is usually thick, whereas the floor of the frontal sinus is separated from the anterior ethmoid cells by thin, bony walls.
2. NATURAL HISTORY
• At the time of diagnosis, most lesions are advanced and commonly involve several adjacent sinuses, the nasal cavity, and often the nasopharynx. See Figure 5-4 for a graphic representation of tumor spread.
• “Ohngren’s line” is an imaginary line originally described in the 1930s, which extends from the medial canthus of the eye to the angle of the mandible. It is a dividing line that can be used to roughly estimate prognosis: tumors inferior or anterior to Ohngren’s line are associated with a better survival rate as they involve fewer critical structures, while lesions superior or posterior to Ohngren’s line tend to have a poorer prognosis because there is a higher likelihood of involving the orbit, optic nerve, ethmoids, pterygopalatine fossa, and carotid artery.
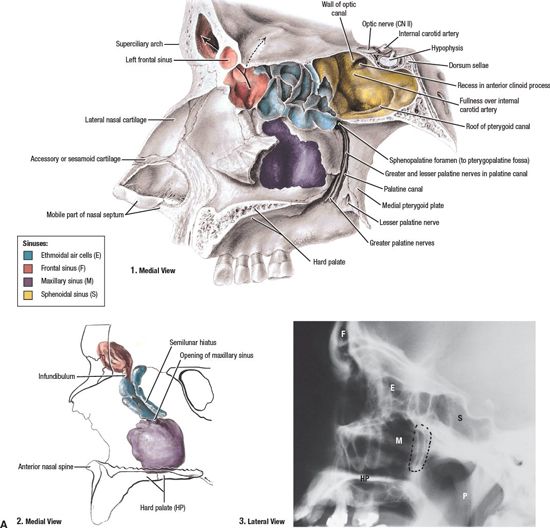
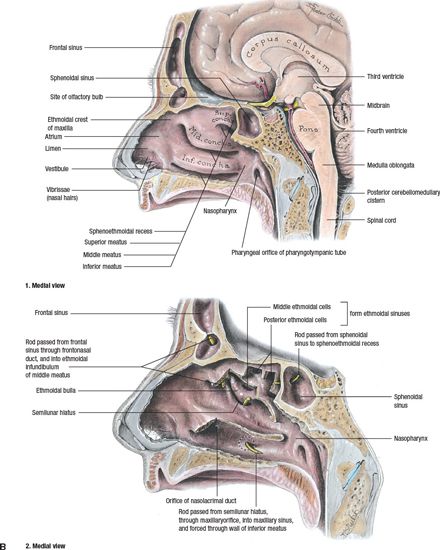
FIGURE 5-1. A-1: Opened sinuses, color coded. A-2: Cast of frontal and maxillary sinuses, color coded. A-3: Lateral radiograph of sinuses. P, pharynx. Dotted outline represents the ptergyopalatine fossa. (From Agur AMR, Dalley AF, eds. Grant’s Atlas of anatomy, 12th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:698, with permission.)
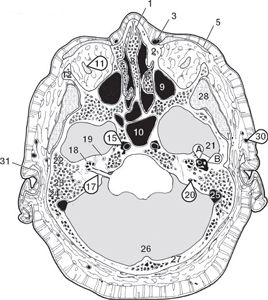
FIGURE 5-2. Inferiormost orbit, and middle and internal ear. Key: 1, Cartilaginous nasal septum; 2, Frontal process of the maxilla; 3, Angular artery; 4, Nasolacrimal duct; 5, Orbicularis oculi muscle; 6, Middle turbinate; 7, Superior turbinate; 8, Perpendicular plate of the ethmoid bone; 9, Maxillary sinus; 10, Sphenoid sinus; 11, Inferior oblique muscle; 12, Frontal process of the zygomatic bone; 13, Zygomatic process of the temporal bone; 14, Sphenoid bone; 15, Internal carotid artery; 16, Cavernous sinus; 17, Cranial nerves VII and VIII; 18, Cochlea of the inner ear; 19, Anterior (superior) semicircular canal; 20, Endolymphatic duct; 21, Ear ossicles (A. stapes; B. malleolarincal joint); 22, Petrous portion of the temporal bone; 23, Mastoid process of the temporal bone; 24, Mastoid air cell; 25, Sigmoid sinus; 26, Falx cerebelli; 27, Occipital bone; 28, Temporalis muscle; 29, Tendon of the temporalis muscle; 30, Superficial temporal vessels; 31, Tragus cartilage of the auricle. (From Dean D, Herbener TE. Cross-Sectional Human Anatomy. Baltimore: Lippincott Williams & Wilkins, 2000.)
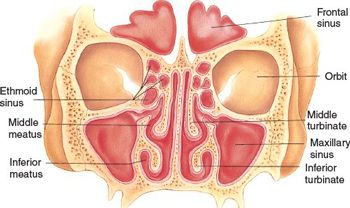
FIGURE 5-3. Cross section of nasal cavity: anterior view. (From Bickley LS, Szilagyi, P. Bates’ Guide to Physical Examination and History Taking, 8th ed. Philadelphia: Lippincott Williams & Wilkins, 2003.)
• There is often orbital invasion from maxillary sinus or ethmoid sinus cancers. Orbital invasion from nasal cavity tumors occurs late.
• The anterior cranial fossa is invaded by way of the cribriform plate and roof of the ethmoid sinuses. The middle cranial fossa is invaded by way of the infratemporal fossa, pterygoid plates, or lateral extension from the sphenoid sinus.
• Lesions involving the olfactory region tend to destroy the septum and may invade the nasal bone, producing expansion of the nasal bridge, and progress to skin invasion.
• Lesions of the anterolateral infrastructure of the maxillary sinus commonly extend through the lateral inferior wall and appear in the oral cavity, where they erode through the maxillary gingiva or into the gingivobuccal sulcus (Fig. 5-5). Tumor that extends posteriorly from the maxillary sinus has immediate access to the base of the skull.
• Lymph node metastases generally do not occur until the tumor has extended to areas that contain abundant capillary lymphatics (Table 5-1). The anterior nasal cavity has the same lymphatic drainage as that of the external nose and tends to drain to the submandibular lymph nodes. The middle and posterior nasal cavity, as well as the paranasal sinuses, drain via the nasopharynx to the retropharyngeal and superior jugulodigastric lymph nodes.
3. DIAGNOSIS AND STAGING SYSTEM
3.1. Signs and Symptoms
• History of recurrent nasal obstruction and recently worsened sinusitis are common symptoms. Minor and intermittent epistaxis may be observed. The mass may protrude from the nose.
• Obstruction of the nasolacrimal system may cause epiphora. Frontal headache, dysosmia (aberration of sense of smell) or anosmia (loss of sense of smell), diplopia, and proptosis secondary to invasion of the orbit are other signs and symptoms that can be observed in paranasal sinus and nasal cavity tumors.
3.2. Physical Examination
• The anterior nasal cavity is inspected by a nasal speculum. A fiberoptic nasoendoscopy must be performed to further evaluate the nasal cavity, sinuses, and nasopharynx. The neck is palpated for adenopathy.
• Cranial nerve examination is very important in paranasal and nasal cavity tumors to evaluate the extension of tumor.
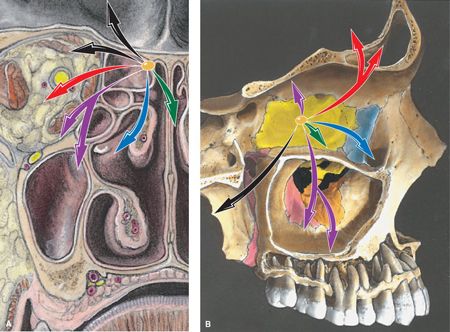
FIGURE 5-4. Patterns of spread. (A) Coronal. (B) Sagittal. The primary cancer (paranasal ethmoid sinus) invades in various directions, which are shown as color-coded vectors (arrows) representing stages of progression: Tis, yellow; T1, green; T2, blue; T3, purple; T4a, red; T4b, black. There are three vectors of invasion: into the orbit; into the nasal passage and paranasal sinuses; and intracranial. (From Rubin P, Hansen JT. TNM Staging Atlas with Oncoanatomy, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2012:21, modified from Agur AMR, Dalley AF, eds. Grant’s Atlas of Anatomy, 12th edition. Philadelphia: Lippincott Williams & Wilkins, 2009.)
3.3. Imaging
• High-resolution sinonasal computed tomography (CT) and magnetic resonance imaging (MRI) should be performed in both the axial and the coronal planes. An attempt should be made to match the imaging planes of both modalities for direct comparison. The anterior skull base, floor of orbit, and cavernous sinus are evaluated on coronal sections. The orbital apex, pterygopalatine fossa, infratemporal fossa, and face are studied on axial sections. Sections must be 3 mm or less in thickness.
• The lymph nodes are not routinely studied in sinonasal cancer. If there is soft tissue, nasopharynx mucosa involvement, or in cases of high-grade lesions, the neck is examined.
• The absence of bone on CT is not necessarily an indication of bone invasion as many bony elements in this region are very thin and easily obliterated.
• Because of the conical shape of the orbit, the maxillary antrum projects into the posteromedial floor of the orbit on axial images.
•
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


