Part 1 Neuro
Case 1

Clinical History
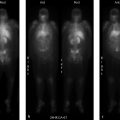
89-year-old male with history of idiopathic normal pressure hydrocephalus and worsening symptoms (▶Fig. 1.1).
Key Finding
Absent CSF flow through ventricular shunt tubing
Top 2 Differential Diagnoses
Shunt obstruction. Ventriculoperitoneal and ventriculoatrial shunts are commonly placed in patients with obstructive hydrocephalus. These shunts are placed percutaneously by neurosurgery. A reservoir, with an internal valve, is placed in the subcutaneous tissues superficial to the skull. Afferent tubing is then passed through the skull and into the ventricular system adjacent to the foramen of Monro. Efferent tubing is connected to the reservoir superficially and courses under the skin and down the neck and chest before terminating within the peritoneal cavity in the abdomen, or extending into the venous system and terminating in the right atrium. Worsening clinical symptoms or increasing ventricular size raises concern for obstruction of the shunt tubing. To evaluate the flow, the reservoir is accessed by the neurosurgical service and a small amount of the patient’s CSF is removed. The dose of In-111 DTPA is then injected into the reservoir in sterile saline, followed by a flush with the previously removed autologous CSF. The efferent tubing can be blocked if evaluation of the afferent tubing is needed. Dynamic imaging is performed for 30 minutes to visualize the flow of CSF. Quantification can be performed by drawing an ROI around the reservoir and measuring the time to half activity, normally 5 minutes or less. Normal examinations should demonstrate flow of activity from the lateral ventricles through the afferent tubing to the reservoir, and then through the efferent tubing to either the peritoneal or venous system. Complete obstruction will show flow of activity into the ventricles and absence of flow into the tubing or reservoir with no terminal destination activity. Possible etiologies for shunt obstruction include injury to the choroid plexus, increasing cellular debris within the CSF, as well as red blood cell and platelet aggregates in patients with intracranial hemorrhage.
Peritoneal pseudocyst. Normally, CSF that drains into the peritoneal cavity is absorbed over time. However, in rare cases a walled-off collection of the drained CSF can form within the peritoneal cavity. This collection is termed a peritoneal CSF pseudocyst which is formed by a wall of fibrous tissue and epithelium. As the cyst grows, backpressure through the peritoneal tubing increases leading to decreased and eventual absent forward flow. If the cyst is imaged early on in its development and growth, focal accumulation of activity within the abdomen is seen. If this diagnosis is suspected and no such accumulation is seen on CSF flow imaging, further imaging with abdominal ultrasound (US) or CT is essential for correct interpretation.
Diagnosis
CSF ventriculoperitoneal shunt tubing obstruction.
✓ Pearls
Normal exams demonstrate flow from the ventricles to either the peritoneal cavity or venous system.
Shunt obstruction will present with absent or delayed antegrade flow.
Peritoneal CSF pseudocyst formation is a rare complication of VP shunt tubing placement.
Cross-sectional imaging is needed if CSF pseudocyst is suspected and flow imaging is negative.
In-111 DTPA is an ideal CSF label. It is nonpyrogenic with a favorable half-life and photon energy.
Suggested Readings
Khan F, Rehman A, Shamim MS, Bari ME. Factors affecting ventriculoperitoneal shunt survival in adult patients. Surg Neurol Int. 2015; 6:25 Mai DT, Vasinrapee P, Cook RE. Diagnosis of abdominal cerebrospinal fluid pseudocyst by scintigraphy. Clin Nucl Med. 1993; 18(3):237–238 Sigg D, Rich R, Ashby S, Jabour B, Glass E. Radionuclide shuntogram demonstrating migration of distal ventriculoperitoneal shunt tubing out of the peritoneal cavity. Clin Nucl Med. 2005; 30(8):552–554Case 2

Key Finding
Absent intracranial activity on a Tc-99m HMPAO scan
Top 3 Differential Diagnoses
Brain death. Brain death is a clinical diagnosis utilizing a combination of physical examination, electroencephalography, and imaging findings. A brain death scan has high specificity as a confirmatory study for absent intracranial perfusion. Scintigraphic imaging can be performed at the patient’s bedside with a portable gamma camera. Imaging may be performed with a nonspecific flow agent (Tc-99m diethylenetriamine pentaacetic acid [DTPA]), or with lipophilic brain perfusion agents (Tc-99m HMPAO or Tc-99m ethyl cysteinate dimer [ECD]) which cross the blood–brain barrier (BBB) and are extracted by viable brain tissue proportional to cerebral flow. A scalp band or tourniquet may be placed around the head to avoid interfering activity from extracranial vessels. The scalp band, however, is contraindicated in pediatric patients due to increased intracranial pressure. First-minute dynamic flow imaging is performed in an anterior projection, with subsequent static blood pool images in both anterior and lateral projections. Delayed SPECT imaging may improve sensitivity in cases where lipophilic agents are utilized. Normal imaging reveals symmetric flow within the anterior and middle cerebral arteries (“trident” sign) on the anterior view, with visualization of dural venous sinuses on blood pool imaging. In brain death, there is termination of carotid activity at the skull base due to increased intracranial pressure overcoming perfusion pressure, thereby shunting blood through the external carotid artery branches projecting over the nasopharyngeal region (“hot nose” sign).
Injection error. Peripheral intravenous injection of the radiotracer is performed as a rapid/tight bolus. A proper bolus is confirmed by visualizing distinct activity within the proximal common carotid arteries. Dose infiltration, slow radiotracer injection, or missed bolus can result in false-positive studies, especially when flow agents (like Tc-99m DTPA, which do not cross the BBB) are used. Tc-99m DTPA is rapidly cleared through renal excretion which allows for reinjection and reimaging in the setting of equivocal or technically limited studies.
Poor radiopharmaceutical labeling/quality control. Quality control is essential with lipophilic brain-specific agents. Poor labeling and instability can result in a false-positive exam. HMPAO should be labeled with fresh eluate within 2 hours of elution. If it is stabilized, it has a shelf life of 4 hours after labeling.
Diagnosis
Brain death.
✓ Pearls
Besides brain death, Tc-99m HMPAO can image cerebral ischemia, seizure focus, and dementia.
Absent intracranial flow and no cerebral/cerebellar uptake of Tc-99m HMPAO confirm brain death.
Brain parenchymal uptake of radiotracer is not seen with flow agents like Tc-99m DTPA.
Scintigraphic evaluation is unaffected by drug intoxication, hypothermia, or metabolic derangements.
Suggested Readings
Conrad GR, Sinha P. Scintigraphy as a confirmatory test of brain death. Semin Nucl Med. 2003; 33(4):312–323 Donohoe KJ, Agrawal G, Frey KA, et al. SNM practice guideline for brain death scintigraphy 2.0. J Nucl Med Technol. 2012; 40(3):198–203 Sinha P, Conrad GR. Scintigraphic confirmation of brain death. Semin Nucl Med. 2012; 42(1):27–32Case 3

Key Finding
Asymmetric decreased uptake within the striatum on I-123 Ioflupane scan
Top 3 Differential Diagnoses
Parkinson’s disease. Parkinson’s disease (PD) is a movement disorder that occurs due to loss of dopaminergic neurons within the substantia nigra. The disease presents after age 60 and includes resting tremor, bradykinesia, rigidity, and loss of balance and coordination. Differentiation between PD and essential tremor (ET) is often difficult. ET is a different tremor disorder of unknown cause that presents with intention or postural tremors, and many patients with ET are misdiagnosed with PD. Recent advances in imaging of the dopaminergic pathways have provided an elegant means of differentiating these two disorders. I-123 Ioflupane (DATscan, GE Healthcare, Chicago, IL) binds to the presynaptic dopamine transporters present at the end of axons of the nigrostriatal pathway that course from the substantia nigra to the striatum. Uptake of this radiopharmaceutical is seen within the striatum itself and not the substantia nigra where the neurons originate. Normal scans demonstrate symmetric uptake within the striata bilaterally, which appear as smooth comma–shaped structures. Abnormal uptake consists of any decrease in uptake and is usually asymmetric.
Dementia with Lewy Bodies. Dementia with Lewy Bodies (DLB) is the second most common neurodegenerative disorder in patients over the age of 65. In contrast to Alzheimer’s disease (AD), memory deficits often present as a later finding, with initial loss of attention and visuospatial function. Still, when presenting with memory deficits, it is sometimes difficult to differentiate these two entities based on symptoms alone. Recent studies have demonstrated a progressive loss of dopaminergic neurons in patients with DLB, representing an important differentiating feature between DLB and AD.
Other parkinsonian syndromes. Other parkinsonian syndromes, such as progressive supranuclear palsy (PSP) and multiple system atrophy (MSA), also involve loss of dopaminergic neurons and will demonstrate similar findings on I-123 Ioflupane scanning. Studies have shown this scan to improve physician confidence in their diagnosis of these syndromes.
Diagnosis
Presynaptic dopaminergic defect within the striatum, consistent with a parkinsonian syndrome in the appropriate clinical setting.
✓ Pearls
I-123 Ioflupane binds to presynaptic dopaminergic transporters within the striatum.
Abnormal scans show loss of comma–shaped striatal uptake with asymmetric decreased uptake.
Abnormal DATscan suggests dopaminergic neurodegenerative disease (PD, PSP, or MSA).
DLB also involves progressive loss of dopaminergic neurons, which differentiates it from AD.
Suggested Readings
Benamer TS, Patterson J, Grosset DG, et al. Accurate differentiation of parkinsonism and essential tremor using visual assessment of [123I]-FP-CIT SPECT imaging: the [123I]-FP-CIT study group. Mov Disord. 2000; 15(3):503–510 Colloby SJ, Williams ED, Burn DJ, Lloyd JJ, McKeith IG, O’Brien JT. Progression of dopaminergic degeneration in dementia with Lewy bodies and Parkinson’s disease with and without dementia assessed using 123I-FP-CIT SPECT. Eur J Nucl Med Mol Imaging. 2005; 32(10):1176–1185 Seifert KD, Wiener JI. The impact of DaTscan on the diagnosis and management of movement disorders: A retrospective study. Am J Neurodegener Dis. 2013; 2(1):29–34Case 4

Clinical History
48-year-old female patient with chronic intractable complex partial epilepsy (▶Fig. 4.1).
Key Finding
Unilateral decreased cerebellar perfusion or metabolism
Top 3 Differential Diagnoses
Crossed cerebellar diaschisis. The term “diaschisis” was originally coined in 1914 by Constantin von Monakow, meaning “shocked throughout” in Greek. Crossed cerebellar diaschisis (CCD) refers to the loss of function within an undamaged part of the cerebellum that is distantly connected to a damaged part of the cerebrum via long axons. This leads to disruption of the corticopontocerebellar tracts, depressed metabolism and blood flow, and eventual cortical atrophy. Given the normal contralateral crossing pattern of cerebral neurons that occurs within the brainstem, connected areas within the cerebellum lose function when areas of the contralateral cerebral cortex are damaged (hence the term “crossed”). As the cerebellum serves the important function of providing coordination of motor impulses, this pattern is often seen following an insult to the motor cortex within the parietal lobe. Possible associated supratentorial pathologies include tumor, seizure focus, and stroke. Similar findings of decreased uptake will be seen on both F-18 FDG PET metabolism imaging and brain perfusion single-photon emission computed tomography (SPECT).
Stroke. Infarcted brain will show little to no metabolism on F-18 FDG positron emission tomography/computed tomography (PET/CT) and decreased perfusion on SPECT imaging, depending on the extent of damage. In these cases, the CT images of the brain are essential for correct interpretation. As with all studies, ensure that all available comparison studies are used as part of the current study interpretation.
Prior surgery. As one would expect, following surgical resection of a portion of the cerebellum (often for tumor), decreased metabolism and perfusion will be seen within the location of the absent cerebellar tissue. It is essential to compare findings with correlative anatomic imaging, available previous studies, as well as the patient’s medical and surgical history.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


