Part 2 Thyroid and Parathyroid
Case 12

Clinical History
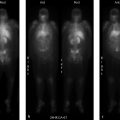
62-year-old male with hyperthyroidism. Laboratory values at time of exam: thyroid stimulating hormone (TSH) < 0.005 µIU/mL (normal 0.270–4.20), free T4 > 5.18 (normal range 0.93–1.7 ng/dL) (▶Fig. 12.1).
Key Finding
Increased thyroid radioiodine uptake in the setting of hyperthyroidism
Top 3 Differential Diagnoses
Graves’ Disease. Graves occurs secondary to thyroid-stimulating antibodies that bind to thyroid-stimulating hormone (TSH) receptors, stimulating the gland to create hormone independent of the central axis. Radioiodine (I-123) scan will show diffuse homogeneous thyroid uptake, possibly a pyramidal lobe, and increased uptake at both 4 and 24 hours. Uptake may be normal at 24 hours in cases of rapid iodine turnover. Normal uptake values are for a euthyroid patient, so “normal” values in a patient with suppressed TSH are not normal and indicate subclinical Graves. I-131 ablation can be used for treatment with dosages generally calculated taking thyroid gland size and 24-hour iodine uptake percentage in account, typically around 12–15 mCi.
Toxic multinodular goiter (TMNG). TMNG occurs when a multinodular goiter develops some autonomous function. Imaging shows an enlarged gland with multiple cold, warm, and hot nodules. Uptake values may be normal or elevated. I-131 ablation is used for treatment, often with 30 mCi.
Hyperfunctioning adenoma. A hyperfunctioning thyroid adenoma may result in hyperthyroidism. Imaging usually demonstrates a single hot nodule with suppression of the rest of the gland. Uptake values may be normal or increased. A hot nodule on Tc-99m pertechnetate should be followed with an I-123 scan to rule out a discordant nodule, as thyroid carcinoma will be hot on a pertechnetate scan. Adenomas may be more resistant to I-131 and are typically ablated with around 30 mCi. Patients may return to a euthyroid state after ablation as the remainder of the thyroid gland is suppressed and may not take up I-131.
Additional Diagnostic Considerations
Hashimoto’s thyroiditis: Radioiodine uptake may be increased early in the disease as the body responds to a drop in thyroid function by increasing TSH production. Patients are rarely imaged in this stage, and hyperthyroidism (Hashitoxicosis) would have been present prior to imaging.
Gestational trophoblastic disease (GTD): Human chorionic gonadotropin (HCG)-secreting GTD can result in hyperthyroidism as HCG is structurally similar to TSH, typically occurs with HCG over 300 IU/mL.
Diagnosis
Graves’ disease.
✓ Pearls
Normal uptake on a thyroid scan is 6–18% at 4–6 hours and 10–30% at 24 hours, in a euthyroid patient.
In Graves’ disease, uptake can be normal at 24 hours in cases of rapid iodine turnover or subclinical disease.
Typical I-131 ablation doses are 15 mCi for Graves and 30 mCi for TMNG and hyperfunctioning adenoma.
It is important to remember that “normal” uptake values are abnormal in the setting of a suppressed TSH.
Suggested Readings
Day TA, Chu A, Hoang KG. Multinodular goiter. Otolaryngol Clin North Am. 2003; 36(1):35–54 Nachiappan AC, Metwalli ZA, Hailey BS, Patel RA, Ostrowski ML, Wynne DM. The thyroid: review of imaging features and biopsy techniques with radiologic-pathologic correlation. Radiographics. 2014; 34(2):276–293 Nayak B, Hodak SP. Hyperthyroidism. Endocrinol Metab Clin North Am. 2007; 36(3):617–656, vCase 13

Clinical History
37-year-old woman with symptomatic and laboratory evidence of thyrotoxicosis (▶Fig. 13.1).
Key Finding
Decreased thyroid uptake in the setting of hyperthyroidism
Top 3 Differential Diagnoses
Subacute thyroiditis. It results from an inflammatory response following a viral illness leading to giant cell infiltration of thyroid follicles. The follicles swell and eventually rupture leading to release of thyroid hormone and thyrotoxicosis. The swelling of the follicles results in the clinical symptoms of a painful and tender thyroid gland. Free thyroid hormone levels are elevated resulting in suppression of thyroid stimulating hormone (TSH) and decreased iodine uptake, also in part due to disruption of the follicular membrane. Treatment is anti-inflammatory medications and, in severe cases, steroids.
Induced thyrotoxicosis. It results when an individual is exposed to excessive amounts of iodine either via medication such as amiodarone or radiographic contrast agents. Normally the Wolff–Chaikoff effect prevents excessive thyroid hormone synthesis during exposure to excessive amounts of iodine. Jod-Basedow phenomenon results when there are autonomous areas within the thyroid gland that produce excessive thyroid hormone with exposure to excessive amounts of iodine resulting in TSH suppression and reduced radioiodine uptake. A recent large iodine load could have a similar effect via competitive inhibition, possibly masking an underlying productive cause of hyperthyroidism, such as Graves’ disease or multinodular goiter.
Struma ovarii. It is a rare ovarian teratoma that contains functioning thyroid tissue. While most cases do not produce a significant amount of thyroid hormone, on rare occasions the exogenous thyroid hormone production can be symptomatic. T3 and T4 levels will be elevated and TSH levels will be suppressed. There will be decreased uptake in the thyroid gland on thyroid scintigraphy due to the production of the ectopic thyroid hormone with increased uptake in the ovarian tumor. The ectopic thyroid tissue is better demonstrated with I-123 than with pertechnetate since urinary excretion of the pertechnetate could obscure the ovarian mass. It is important to image the pelvis in a female patient sent for hyperthyroid evaluation with decreased iodine uptake in the neck to exclude this diagnosis.
Additional Differential Diagnoses
Thyrotoxicosis factitia: It is thyrotoxicosis caused by exogenous thyroid hormone administration, either knowingly or unknowingly. There will be elevation of serum T3 and T4 levels, often with a higher serum T4/T3 ratio than in endogenous thyrotoxicosis, since the exogenous hormone is often pure T4, and there will be decreased uptake on scintigraphy due to suppressed TSH. Serum thyroglobulin (Tg) level will be very low or undetectable with thyrotoxicosis factitia.
Diagnosis
Subacute thyroiditis.
✓ Pearls
Subacute thyroiditis will have a history of recent viral illness and a tender, enlarged thyroid.
There will be a history of recent exposure to iodine (contrast, medications) with induced thyrotoxicosis.
Suspect struma ovarii with a pelvic mass and decreased thyroid uptake in the setting of hyperthyroidism.
Serum Tg levels will be very low/undetectable with thyrotoxicosis factitia.
Suggested Readings
Dujardin MI, Sekhri P, Turnbull LW. Struma ovarii: role of imaging? Insights Imaging. 2014; 5(1):41–51 Intenzo CM, dePapp AE, Jabbour S, Miller JL, Kim SM, Capuzzi DM. Scintigraphic manifestations of thyrotoxicosis. Radiographics. 2003; 23(4):857–869 Mittra ES, Niederkohr RD, Rodriguez C, El-Maghraby T, McDougall IR. Uncommon causes of thyrotoxicosis. J Nucl Med. 2008; 49(2):265–278Case 14

Clinical History
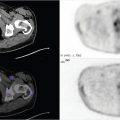
63-year-old male with solitary 2-cm right thyroid nodule and long history of labs consistent with subclinical hyperthyroidism (▶Fig. 14.1).
Key Finding
Cold nodule on I-123 thyroid scan
Top 3 Differential Diagnoses
Thyroid carcinoma. Ultrasound and fine needle aspiration (FNA) are the primary diagnostic procedures for thyroid nodule in a euthyroid patient. Nuclear medicine thyroid imaging for nodule characterization should be reserved for patients with hyperthyroidism (suppressed TSH), or an indeterminate biopsy. Cold or nonfunctioning nodules on I-123 thyroid scans are nonspecific and may represent colloid cyst (40%), nonfunctioning adenoma (40%), or thyroid carcinoma (15–20%). The incidence of cancer is lower (< 5%) in the setting of multinodular goiter. Hot or hyperfunctioning nodules on I-123 scan, defined as uptake in the nodule suppressing the rest of the thyroid gland, are essentially always benign. However, a hot nodule on pertechnetate scan requires further evaluation with I-123 scan to exclude a discordant nodule, which requires FNA to exclude thyroid carcinoma. Risk factors for thyroid malignancy include age < 20 or > 60 years, male patient, family history, prior radiation therapy to the head/neck, and/or a dominant nodule with concerning ultrasound features (solid, hypoechoic, hypervascular nodule with microcalcifications). Papillary carcinoma is the most common subtype, followed by follicular. Medullary and anaplastic carcinomas are less common and highly aggressive. Treatment of localized thyroid carcinoma typically consists of total thyroidectomy followed by I-131 ablation therapy. Patients are followed with thyroglobulin (Tg) levels, as well as whole-body I-131 imaging, for at least 2 years after radioiodine ablation (RIA).
Colloid cyst. These are benign localized follicles filled with gelatinous colloid. They usually originate from cystic degeneration of thyroid adenomas and are hyperintense on T1-weighted MRI due to high protein content. Ultrasound characteristics include a cystic lesion with inspissated colloid, which is hyperechoic and demonstrates ring-down or comet tail artifact.
Nonfunctioning adenoma. Thyroid adenomas are benign lesions that may be functioning (hot nodule) or nonfunctioning (cold nodule). They can be multiple in the setting of multinodular goiter. On ultrasound, benign adenomas are typically well encapsulated with a hypoechoic halo. Interval growth is not unusual. A dominant hyperfunctioning adenoma with suppression of the remainder of the gland in the setting of hyperthyroidism is called an autonomous nodule (produces thyroid hormones independent of TSH). Multinodular goiter and autonomous nodules are generally more resistant to ablation therapy than Graves’ disease; hence, these patients are treated with higher doses of I-131 (about 30 mCi).
Diagnosis
Nonfunctioning adenoma.
✓ Pearls
I-123 thyroid scan is indicated in hyperthyroidism or nodule evaluation after an indeterminate biopsy.
A cold nodule may be a colloid cyst (40%), nonfunctioning adenoma (40%), or thyroid cancer (15–20%).
A hot nodule on Tc pertechnetate may be cold or “discordant” on I-123 (trapping without organification).
Papillary and follicular cancers are amenable to I-131 ablation, medullary and anaplastic carcinomas are not.
Suggested Readings
Intenzo CM, Dam HQ, Manzone TA, Kim SM. Imaging of the thyroid in benign and malignant disease. Semin Nucl Med. 2012; 42(1):49–61 Nachiappan AC, Metwalli ZA, Hailey BS, Patel RA, Ostrowski ML, Wynne DM. The thyroid: review of imaging features and biopsy techniques with radiologic-pathologic correlation. Radiographics. 2014; 34(2):276–293 Yeung MJ, Serpell JW. Management of the solitary thyroid nodule. Oncologist. 2008; 13(2):105–112Case 15

Key Finding
Focal area of increased uptake on radioiodine thyroid scan with washout of the rest of the thyroid gland
Top 2 Differential Diagnoses
Toxic adenoma. Radioiodine thyroid uptake and scan is most frequently performed for the evaluation of hyperthyroidism. However, the study can also be useful for the evaluation of a thyroid nodule, particularly in the setting of an indeterminate biopsy with concerning imaging features. A “hot” nodule on thyroid scintigraphy will appear as a focal area of increased radioiodine uptake with washout of the remaining thyroid gland. This is reassuring of benignity as this appearance is nearly pathognomic for a hyperfunctioning, or toxic, thyroid adenoma. A true hot nodule has a very low chance of being malignant as even well-differentiated carcinomas are rarely hyperfunctioning. The washout of the remaining thyroid gland is an important feature because it proves that the nodule is producing thyroid hormone independently while the remaining gland is responding appropriately to the central axis. The autonomous nature of toxic adenomas is thought to be due to the mutation of the TSH receptors resulting in continuous activation. Toxic adenomas can be treated with I-131 ablation, usually utilizing a 30-mCi dose. Patients who receive radioiodine ablation (RIA) may end up euthyroid and without the need for thyroid hormone replacement as the appropriately suppressed iodine uptake of the remaining thyroid gland can be protective.
Thyroid carcinoma. It most commonly presents as a cold nodule on thyroid scintigraphy performed with radioiodine. However, while it is rare, thyroid carcinoma can present with the ability to trap and organify iodine independent of the central axis. This occurs in well-differentiated cancers, and even when present they are rarely hyperfunctioning to the point of resulting in clinical hyperthyroidism. However, as a “hot” nodule is not definitively benign, a nodule that has imaging characteristics which meet criteria for biopsy per standard guidelines should be biopsied regardless of radioiodine thyroid scan findings.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


