Cardiac cirrhosis: Flattening of Doppler wave form in hepatic veins
“To and fro” motion in hepatic veins and IVC
TOP DIFFERENTIAL DIAGNOSES
• Budd-Chiari syndrome
• Hepatic cirrhosis
• Acute viral hepatitis
CLINICAL ISSUES
• Passive hepatic congestion usually secondary to
Congestive heart failure
Constrictive pericarditis
Tricuspid insufficiency
Right heart failure
• Radiologists may be 1st to recognize cardiac source of liver disease
• Diagnosis is based on clinical and imaging findings
DIAGNOSTIC CHECKLIST
• Differentiate acute passive hepatic congestion from Budd-Chiari and viral hepatitis
• Distinguish chronic, cardiac cirrhosis from other etiologies
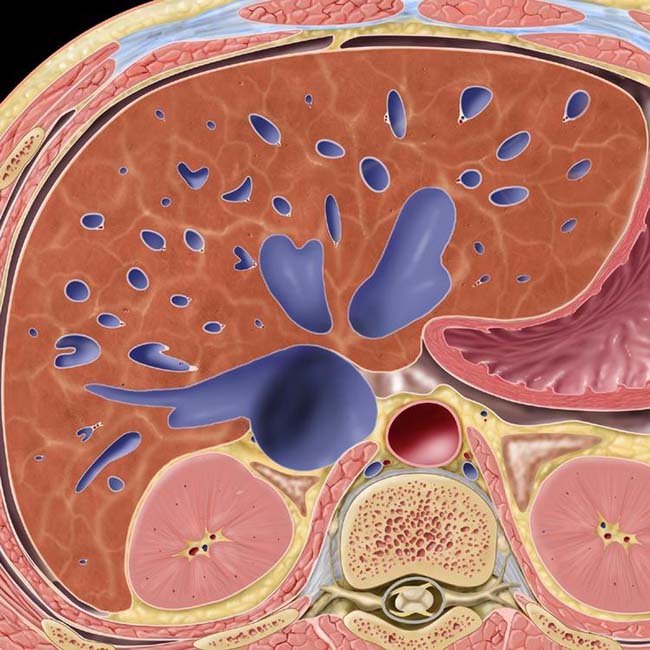
(Left) Graphic shows massive diffuse dilatation of the hepatic veins and mildly heterogeneous liver parenchyma due to passive congestion of the liver.
(Right) Axial CECT in the arterial phase shows early retrograde opacification of dilated hepatic veins and the inferior vena cava (IVC) due to reflux of injected contrast medium through the heart, a sign of impaired antegrade hepatic venous drainage.
(Left) Increased pulsatility of portal vein Doppler signal is demonstrated in this patient with passive hepatic congestion secondary to tricuspid insufficiency.
(Right) Transverse ultrasound shows dilated hepatic veins and IVC in a patient with passive hepatic congestion.
TERMINOLOGY
Synonyms
• Congested liver in cardiac disease
Definitions
• Stasis of blood within liver parenchyma as result of impaired hepatic venous drainage
IMAGING
General Features
• Best diagnostic clue
Dilated hepatic veins with “to and fro” blood flow on color Doppler US










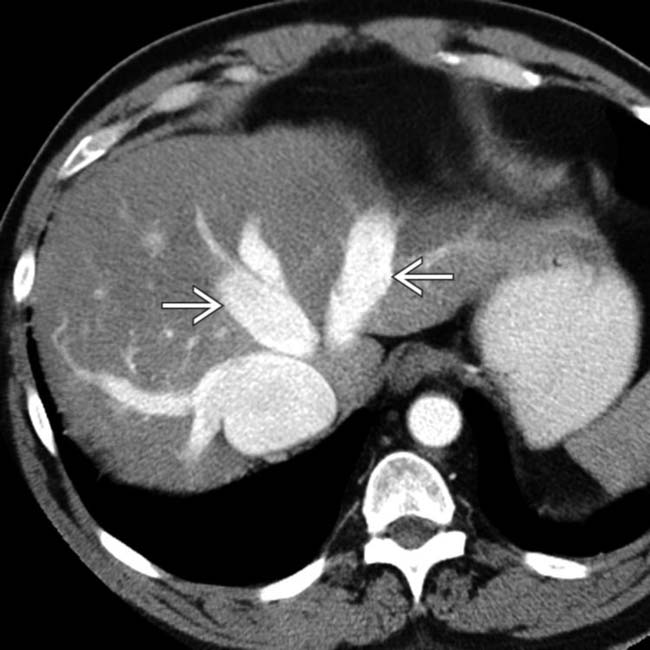
 and the inferior vena cava (IVC) due to reflux of injected contrast medium through the heart, a sign of impaired antegrade hepatic venous drainage.
and the inferior vena cava (IVC) due to reflux of injected contrast medium through the heart, a sign of impaired antegrade hepatic venous drainage.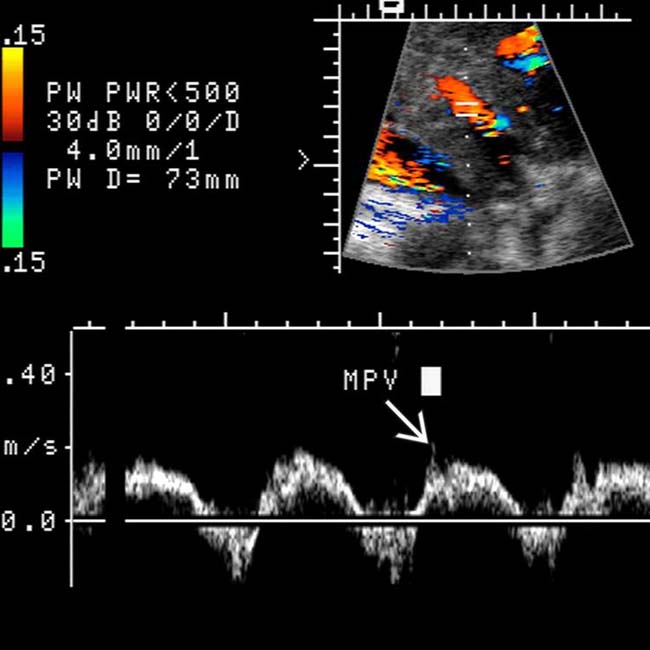
 is demonstrated in this patient with passive hepatic congestion secondary to tricuspid insufficiency.
is demonstrated in this patient with passive hepatic congestion secondary to tricuspid insufficiency.
 and IVC in a patient with passive hepatic congestion.
and IVC in a patient with passive hepatic congestion.



















