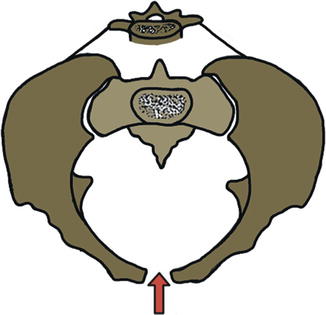
Scheme 20.1
Representation of the “posterior tension band” comparable to a “suspension bridge” where the sacrum represents the horizontal component (red arrow) and the iliolumbar ligaments as additional stabilizing elements that join the iliac crest to the transverse process of the fourth and fifth lumbar vertebrae (black arrow)
The pelvic ring rotational stability is possible by ligaments with a transverse-horizontal course (the anterior sacroiliac; the posterior sacroiliac “short” horizontal component; the sacrospinous, a strong ligamentous band extended from the posterior surface of the sacrum to the ischial spines; and the iliolumbar), which are opposed to the external rotation of the pelvis.
The vertical stability is possible by ligaments with a vertical course (the sacrotuberous extended from the posterior surface of the sacroiliac complex to the ischial tuberosity and the posterior sacroiliac “long” vertical component), which are opposed to vertical and multidirectional dislocation.
Conceptually, it is important to remember, because of its particular ring constitution, that for each injury caused by the action of a high-energy force vector in one area, it must always correspond to another bone or ligamentous lesion on the opposite side [9, 25, 26] (Scheme 20.2).
Scheme 20.2
The pelvic ring constitution demonstrates that for each injury caused by the action of a high-energy force vector in one area, it must always correspond another lesion on the opposite side
Exceptions to this rule are insufficiency fractures, due to trauma caused by “low-energy” force vectors, as it occurs in osteoporotic patients, in some stress fractures, or in avulsion fractures typical of adolescent sport injuries.
Avulsion fractures are common in young athletes aged between 11 and 16 years with predominance in males. They usually occur in a locus minoris resistentiae, represented by the insertion of the tendons at the level of the apophysis that are secondary ossification centers before the fusion. They are mostly composed by cartilage.
20.3 Classification
Pelvic ring fractures may be classified into two subtypes based on the trauma energy.
Low-energy traumas are represented by stable fractures, which do not interrupt the continuity of the ring and are less frequently associated with complications.
High-energy traumas determine a significant anatomical alteration and are therefore potentially associated with severe complications, representing one of the fundamental challenges in the clinical and therapeutic management of major polytraumatized patients.
The PRD represents historically an important dilemma, both clinically and diagnostically, and for the therapeutic decision. The fractures are characterized by a great variety of very different kinds of injuries from anatomical and clinical point of view, as a “grayscale,” which may include at one end of the spectrum a stable intact pelvic ring and at the other part a completely unstable pelvis.
The radiologist will assess which part of the spectrum will place the single type of fracture.
The management of a polytrauma patient with pelvic fracture is based on clinical and hemodynamic conditions and on the degree of pelvic instability, which can be well understood through the analysis of the injury mechanism [8].
If the stability is the key, analyzing the combination of individual anterior and posterior injuries, with a particular focus to the posterior one, will carryout an accurate radiological evaluation. The instability condition depends essentially on the degree of involvement of the posterior tension band.
There are historically known different classification systems proposed by many authors [27], often articulated in different and poorly standardized modality.
The technological revolution determined by the use and the increasing availability of CT and then the spiral and spiral multi-slices scans, in addition to the evolution of surgical and orthopedic instruments, has profoundly changed the treatment approach with a higher number of surgical operations compared to conservative therapy.
Classification systems should be used as tools to help determine prognosis, to direct the search of complications, and to guide for the most appropriate treatment.
The traditional classification systems are based mainly on the definition of the degree of instability of the pelvic ring. The fundamental assumption was that the more unstable the fracture, the greater the risk of complications, especially hemorrhagic [19]. This undoubtedly logical and correct principle was subsequently dismissed by some authors [28] because of the poor diagnostic impact of the principal classification system especially on the search of vascular complications, which could not be present in fractures with an important dislocation of osseous components, often occuring in other less significant fractures.
The modern history of pelvic fracture management begins with iliac wing fracture reported by Duverney in 1751 (Duverney’s fracture), from the French surgeon Joseph-Franҫois Malgaigne in 1859, with the clinical description of “double vertical” and shear shaped, known as “Malgaigne’s fracture,” as a combination of pubic rami and iliac wing fractures [5].
Watson-Jones, in 1937, first defined and classified the fractures based on the location of the fracture.
Connoly and Hedberg, in 1969, focused on the concept of stability and the importance of the biomechanical integrity of the posterior pelvis.
Bucholz clarifies the concepts based on the importance of the anterior pelvic ring than the posterior and on the search of the no detectable injuries of the posterior side.
He provides pathological demonstration that double injury to the pelvic ring is the rule confirming the presence of a posterior lesion in all his victims of fatal motor vehicle accidents at the time of medicolegal autopsy; lesions are graded as type I, type II, or type III depending on the degree of instability [29].
Huittinen and Slatis study pelvic patho-anatomy and are the first who note the relationship between the force energies of impact (high- versus low-energy injuries).
The Looser and Crombie classification takes into consideration both anterior and posterior components of pelvic injury.
Trunkey introduces the concept of stability, adding the terms “comminuted,” “stable,” and “unstable” in grading pelvic fracture.
Classic anatomic and biomechanical studies in pelvic disruption, performed during the mid-twentieth century by a Canadian surgeon George Pennal, are a fundamental contribution, and he is the first one who analyzes in detail the basic mechanism of pelvic injury. The classification system recognizes three mechanisms of direction of force action, which determine injuries: anterior-posterior compression (APC), lateral compression (LC), and “vertical shear” (VS) [5, 9].
During this period, the management of pelvic fracture is generally nonoperative with poor clinical outcome and post-traumatic secondary orthopedic and neurological complications.
Tile classification greatly appreciated by orthopedists uses an alphanumeric criterion based on the assessment of stability of the posterior arch (sacroiliac complex) with the purpose of harmonizing the therapeutic and prognostic management of fractures. It divides the pelvis into the posterior arch (posterior to the acetabulum) and the anterior arch (anterior to the acetabulum), with a spectrum ranging from stable injuries to unstable fractures; each type is divided into three types [1–4]:
Type A [1–3]: Stable and the posterior part of the ring is intact; generally nonoperative management—NOM (avulsion fractures, iliac wing fractures, fractures of the sacrum or coccyx).
Type B [1–3]: Vertically stable but rotationally unstable or partially stable, secondary to an incomplete disruption of the posterior arch structures; these include an external rotation of so-called open-book-type fractures (APC) with disruption of the anterior pelvic arch through the symphysis pubis or through the rami and internal rotation LC injuries with a combination of anterior and posterior arch fractures.
Acetabular fractures are considered separately in the classifications of Tile [30].
A fundamental concept both in clinical and radiological management is to speak generally of pelvic fracture but to distinguish a PRD from an acetabulum fracture.
The polytraumatized patient with a pelvic ring fracture, for the complex clinical problems and consequently more complex management issues, is profoundly different from an acetabular fracture patient, whose problems are mainly orthopedic.
A fracture of the acetabulum is even so associated with pelvic ring fracture in a variable percentage from 15 to 20% of cases.
The American Orthopedic Trauma Association (OTA)/AO (Association for Osteosynthesis) pelvic fracture classification is an alphanumerical and more comprehensive classification system designed to standardize and more accurately report various fracture patterns.
The AO/OTA classification of pelvic ring fractures is divided in three groups (A, B, C) and in relative subgroups [1–3] with increased instability.
Type A fractures are lesion sparing (avulsion fractures of the innominate bone, fractures of the sacrum and coccyx). Type B fractures, with incomplete, unilateral disruption of the posterior arch, are partially stable (external rotation, APC with open-book-type injury; internal rotation, LC injury). Type C fractures are totally unstable, secondary to complete disruption of the posterior arch, and are more commonly seen in the younger patient population.
This classification describes accurately specific fracture patterns and is useful for research purposes but relatively less practical for routine use [5, 31].
The classification of Young revisited by Burgess combines the concepts of the two classifications of Tile and Pennal and is therefore extremely useful in finding the associated complications. Tile’s criteria concern the stability, while Pennal’s criteria concern comprehension of the mechanism of action. It is currently the most widely used system reported in the orthopedic literature.
These criteria, through the stratification of the grade of force vector of injury, represent a valid tool in the management of the patient in the emergency room.
The classification of Young revisited by Burgess is based on the direction and on the grade of force vector energy of the lesion, determining a gradual severity on the compression fractures that are classified in four types with growing instability: lateral compression, LC; anterior-posterior compression, APC; vertical shear, VS; and combined mechanism injury, CM [1, 4, 7, 9, 24, 30–35].
Lateral compression (LC) fractures: The “implosion type” (LC1, LC2, LC3).
The most frequent. Represent 59% of fractures. The force vector acts in lateral direction, resulting in an internal rotation of the injured hemi-pelvis. The ilium rotates medially.
In these fractures the sacrospinous and sacrotuberous ligaments are shortened determining a reduction of the transverse diameter of the entire pelvis and a possible overlap of the pubic branches with the appearance of blocked symphysis classically defined as a “lock” (“locked symphysis”) (Scheme 20.3) (Fig. 20.1).
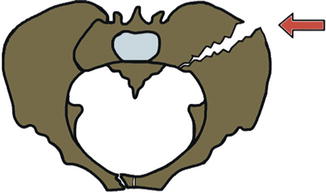
Scheme 20.3
Figure of lateral compression fracture (LC) with force vector that acts in lateral direction, resulting in an internal rotation of the injured hemi-pelvis and the possibility of overlap of the pubic branches with the appearance of blocked symphysis (“locked symphysis”)
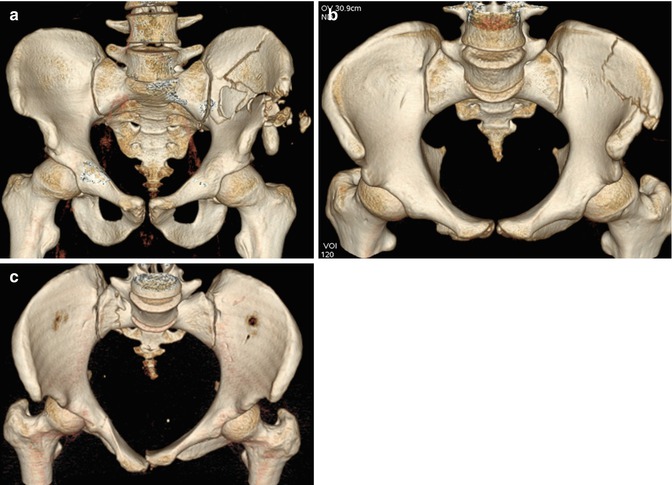
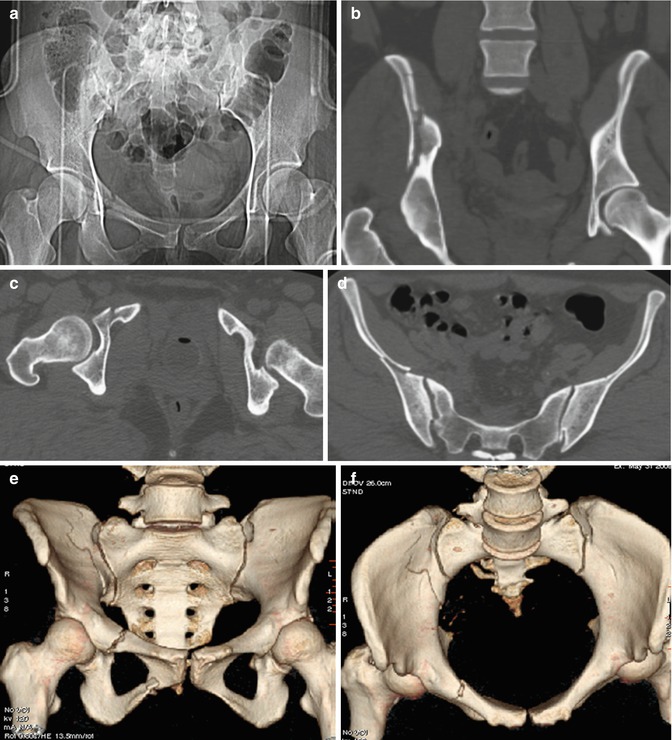
Fig. 20.1
(a–c) Lateral compression fractures (LC), type I. (a, b) CT 3D (VR) reconstruction AP and inlet view show lateral force vector, resulting in fracture of the left iliac wing on the side of the impact. (c) CT 3D (VR) reconstruction inlet view shows a “locked symphysis” fracture due to the overlap of the pubic branches with appearance of blocked symphysis. In these fractures the lesions of sacrospinous and sacrotuberous ligaments determine a reduction of the transverse diameter of the entire pelvis
Usually you can find a transverse fracture of pubic rami ipsilateral or contralateral to the posterior injury.
Four different combinations of the anterior pelvic ring fractures are described (unilateral of both branches, unilateral of both branches + symphysis, both branches bilateral, both branches bilateral + symphysis).
The reduction of the pelvis’ transverse diameter, with a consequent reduction of compliance, justifies its potential association with vascular complications, even if severe vascular lesions can result in direct action of a fragment that acts on vascular structures.
Visceral lesions, especially of the bladder, frequently complicate fractures for direct action of pubic disassembled and dislocated element fragments on the anterior wall.
In higher degrees of injury (LC1 + APC or LC2 + APC), the lateral compression force on the impact site is associated with a destructive force by anterior-posterior contralateral compression with a type of mechanism of “rollover,” resulting in a multidirectional instability (“windswept pelvis”).
LC1: Internal rotation. Stable. Associated sacral compression fracture on side of impact. Intact tension bands. Transverse fractures of the pubic rami. It is the most common pelvic fracture pattern, often associated with lower-energy injury mechanism (Fig. 20.2).
LC2: Internal rotation. Unstable internal rotation. Crescent posterior iliac wing fracture on the side of impact and posterior diastasis of the sacroiliac joint (Fig. 20.3).
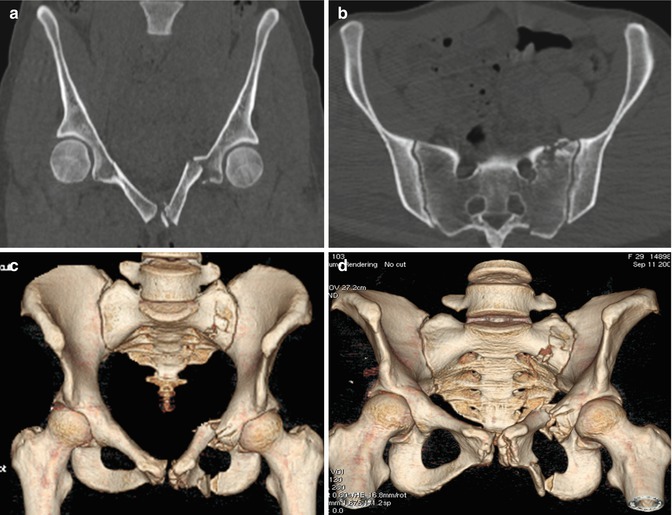
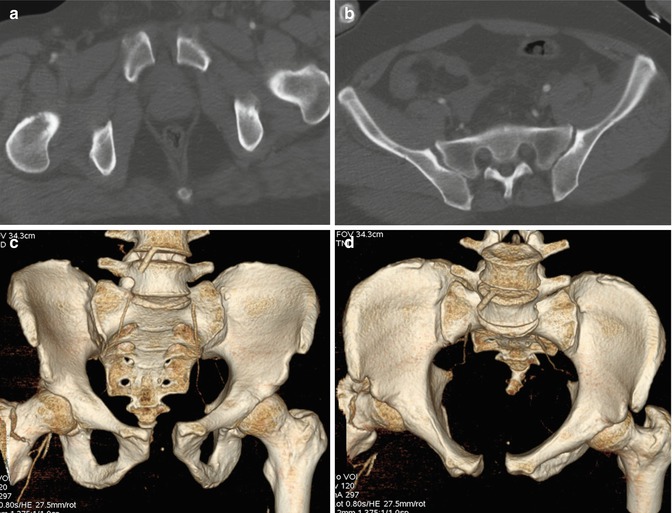
Fig. 20.2
(a–d) Lateral compression fractures (LC), type I stable. (a) CT coronal view shows the horizontal fracture of the left pubic branch on the side of the impact; (b) CT axial view depicts the omolateral compression fracture of the sacrum. (c) CT 3D (VR) reconstruction AP view shows the fracture of left pubic branch; (d) CT 3D (VR) reconstruction outlet view demonstrates the omolateral fracture of the sacrum
Fig. 20.3
(a–f) Lateral compression fractures (LC), type II unstable. (a) Scout view, CT scan MPR coronal view (b), and CT axial view show posterior iliac wing fracture (b, d) on the side of the impact and posterior diastasis of the sacroiliac joint (d). CT 3D (VR) reconstruction AP view (c) and inlet view (d) well depicting fractures of the right pubic branch, right iliac wing, and the posterior diastasis of the homolateral sacroiliac joint
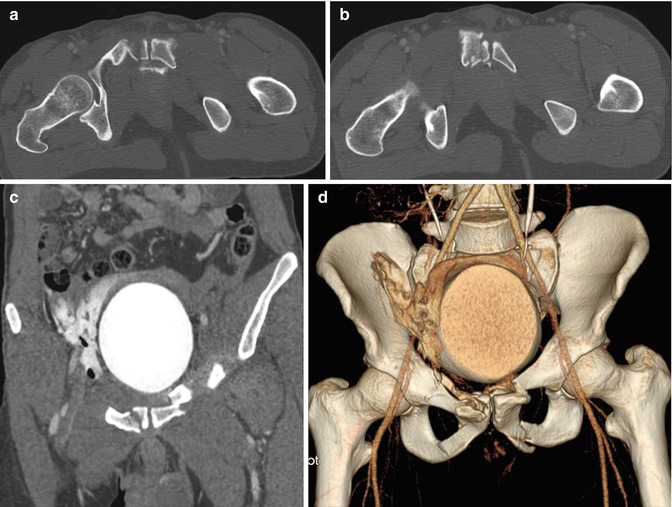
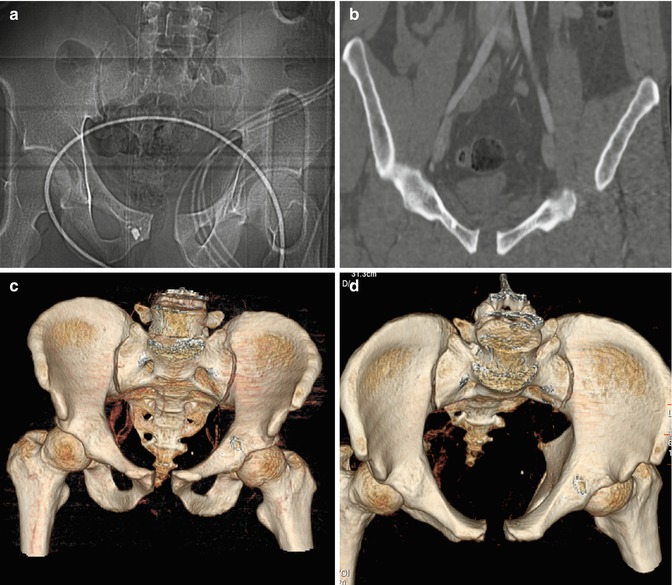
Fig. 20.4
(a–d) Lateral compression fractures (LC), type III unstable. (a, b) CT coronal view shows the fractures of the pubic branches on the impact side and the lateral compression fracture on the opposite side. (c) CT coronal view shows the dislocation of a fragment of the left pubic branch (white arrow) that results in a direct lesion on the bladder with evident iodinated urinary extravasations
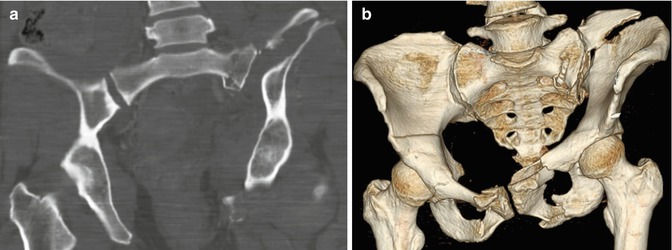
Fig. 20.5
(a–b) Lateral compression fracture (LC), type III. “Windswept pelvis.” CT scan MPR coronal view (a) and CT 3D (VR) reconstruction AP view (b) show pubic branch fractures on the impact side and lateral compression fracture on the opposite side. In these fractures a complete destruction of the back tension band occurs, resulting in both rotational and vertical instability
Anterior-posterior compression (APC) fractures: The so-called open-book fractures (APC1, APC2, APC3). Represent 21% of fractures.
The force vector acts in anterior-posterior direction on the anterior pelvis, the pubic symphysis, and the anterior or posterior superior iliac spines, determining an external rotation of the pelvis.
It is divided into three subgroups with a growing instability, which depends on energy force trauma and on the degree of involvement of the posterior sacroiliac complex and of the sacrospinous and sacrotuberous ligaments (Scheme 20.4).
Scheme 20.4
Figure of an anterior-posterior compression fracture (APC) with force vector that acts in anterior-posterior direction on the pubic symphysis and the anterior or posterior superior iliac spines, resulting in an external rotation of the pelvis with diastasis of the pubic symphysis and the sacroiliac joints
The true pelvis can be compared to a conical sphere. The compression fracture can theoretically increase the radius of the sphere and consequently the pelvic volume, up to tripling or quadrupling consequently the compliance. This is the reason why the so-called open-book fractures must be promptly treated with circumferential compression by tensile strength, even the simplest (pelvic sheet wrap), to normalize the pelvic diameter and consequently the compliance, because hemorrhage is a threatening risk for life.
External rotation of the hemi-pelvis can increase the volume of the pelvic cavity, up to tripling the compliance, with possible potential serious hemodynamic complications from occult bleeding if not identified and promptly treated.
They can determine, due to the diastasis, bladder lesions or specifically of the urethra (straddle fracture) and alterations of the penile shaft vasculature and its innervations with impotence (37% of patients) as the result of nervi erigentes injury. Basta and associates [5, 36] have observed that the probability of urethra lesion becomes higher with increasing of the pubic diastasis: each millimeter of pubic diastasis or inferomedial pubic bone fracture fragment displacement is associated with a 10% increased risk.
Pathognomonic findings of these fractures are represented by the pubic symphysis diastasis, expression of instability if greater than 1 cm, and expression of the contemporary lesion of the sacroiliac synchondrosis when greater than 2.5 cm.
Vertical fracture lines are evident at the level of the pubic rami.
APC1: External rotation. Stable. Little widening (>1 < 2.5 cm) of the pubic symphysis, stretched but intact anterior component of sacroiliac joint, intact posterior ligamentous complex, sometimes minimal diastasis of the sacroiliac synchondrosis, and vertical fracture of one or more pubic rami (Fig. 20.6)
APC2: External rotation. Rotational instability. Widening (>2.5 cm) of the pubic symphysis; diastasis of the anterior component of sacroiliac joint with disrupted sacrotuberous and sacrospinous ligaments; intact posterior ligamentous complex, which maintains a residual condition of stability, like the binding of the book. Unilateral or bilateral. Vertical fracture of one or more pubic rami (Fig. 20.7)
APC3: External rotation with so-called open book. Complete rotational instability. Diastasis (>2.5 cm) of the pubic symphysis; uni- or bilateral sacroiliac dislocation; disrupted posterior ligamentous complex, dissociated from the sacrum, determining the condition of instability with splaying of the anterior arch. Vertical fracture of one or more pubic rami
Fig. 20.6
(a–d) Anterior-posterior compression (APC) fracture, type I. (a) Scout view and CT scan MPR coronal view (b); CT 3D (VR) reconstruction AP view (c) and inlet view (d) demonstrate pubic symphysis diastasis <2.5 cm. These fractures are stable; the back tension band is intact
Fig. 20.7
(a–d) Anterior-posterior compression (APC) fracture, type II. (a–c) CT axial view (a) and CT 3D (VR) reconstruction AP view (c) show diastasis of the pubic symphysis >2.5 cm; (b, d) axial view (b) and CT 3D (VR) reconstruction inlet view well depicting the widening of the right sacroiliac joint. These fractures are rotationally unstable
In this type of fracture, when posterior sacroiliac joint is disrupted, instability is determined.
In these kinds of patients, the association with vascular (and neural) complications is very frequent (Figs. 20.8 and 20.9).
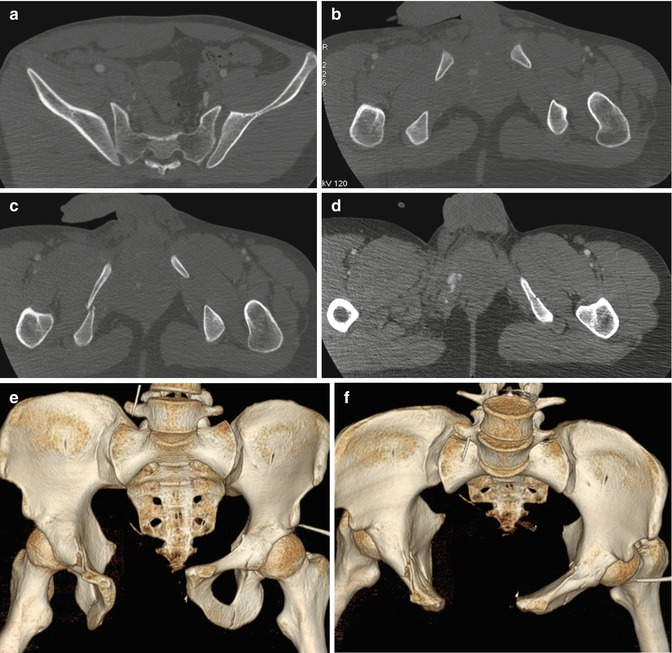
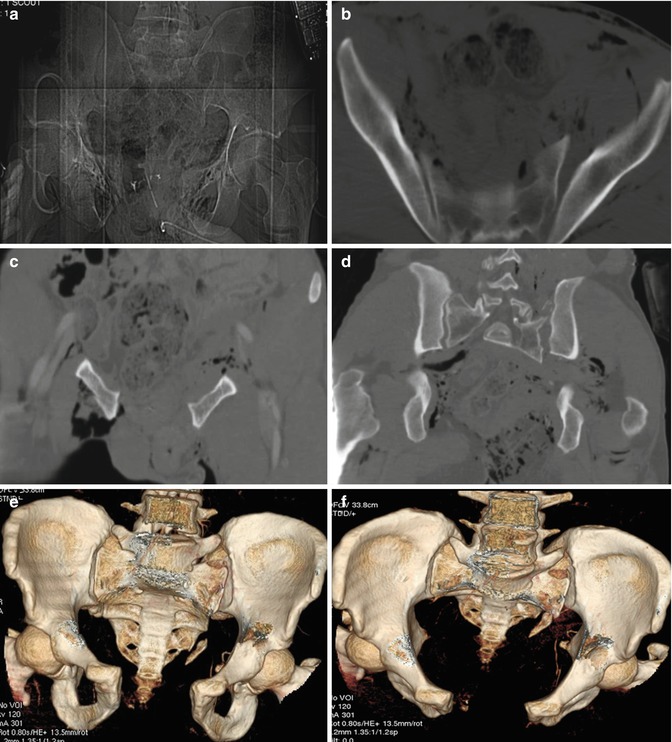
Fig. 20.8
(a–f) Anterior-posterior compression (APC) fracture, type III. “Open-book” fracture with instability condition. (a–d) CT axial view demonstrates widening of both sacral-iliac joints (a), pubic symphysis diastasis >2.5 cm, (b) and vertical fractures of both pubic rami (c, d); (e) CT 3D (VR) reconstruction AP view and CT 3D (VR) reconstruction inlet view (f) show better the diastasis of the pubic symphysis >2.5 cm and the widening of both sacroiliac joints
Fig. 20.9
(a–f) Anterior-posterior compression (APC) fracture, type III. (a) CT scout view; (b) CT axial view; (c, d) CT coronal view. Pubic symphysis diastasis >2.5 cm (a, c) and widening of both sacroiliac joints with dislocation of the left sacroiliac joint are evident (b, d). “Open-book” fracture with instability condition. These fractures are called “open” when they exist in a continuous solution between the fracture site and the skin with soft tissue involvement (b–d). CT 3D (VR) reconstruction AP view (e) and CT 3D (VR) reconstruction inlet view (f) well depicting pubic symphysis diastasis, vertical fractures of both pubic rami, and dislocation of the left sacroiliac joint. Instability condition is due to a complete destruction of the back tension band, resulting in both rotational and vertical instability
Vertical shear (VS): Malgaigne’s or straddle fracture.
Highly unstable. Represent 7% of lesions.
The vector acts in vertical direction (shearing forces), resulting in the destruction of the pelvic ring and of the posterior tension band with dislocation of sacroiliac complex (Scheme 20.5).
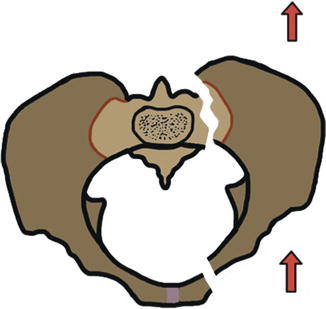
Scheme 20.5
Figure of a vertical shear fracture (VS) with force vector that acts in vertical direction, resulting in the disruption of the pelvic ring and of the posterior tension band with cranial dislocation of the injured hemi-pelvis
Their main characteristic is the involvement of the posterior pelvic elements, represented by vertically oriented sacral fractures (Wallnerfractures), transforaminal or lateral to the foramina; sacroiliac fractures/dislocations; the typical fracture of Malgaigne, in which the posterior fractured element is the iliac wing; or straddle fracture with fracture of both superior and inferior pubic rami (often there is 40% injuries of the genitourinary tract) [29].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


