Chapter 28 In the cerebrovascular literature, perfusion imaging refers to an all-encompassing term of various methods to measure hemodynamically derived functional parameters in the brain.1,2 In radiology, the three most common parameters that are assessed and utilized clinically are cerebral blood volume (CBV), cerebral blood flow (CBF), and mean transit time (MTT). CBV refers to the amount (volume) of blood within a given mass of brain tissue at a given time and is measured in mL/100 g. CBF refers to the flow of blood through an area of the brain and is usually measured in mL/100 g of brain tissue per minute. MTT refers to the time it takes for blood to flow between the arterial inflow and venous outflow in the brain, that is, the time that blood spends in the cerebral capillary circulation, and is often measured in seconds. The general relationship between these three parameters is depicted by the central volume theorem: Evaluation of these various perfusion parameters can give us an understanding of the physiological state of the brain and cerebral vasculature in various disorders and help in patient management. Cerebral perfusion can be measured by a variety of methods including magnetic resonance imaging (MRI), computed tomography (CT), and nuclear medicine techniques. These techniques differ in terms of image acquisition duration, spatial resolution, the types of endogenous or exogenous tracers used, and their ability or accuracy in measuring different perfusion parameters.1 The clinical applications of perfusion imaging include investigation of cerebrovascular disease, brain tumors, and the effect of other diseases on cerebral perfusion. Dynamic susceptibility contrast (DSC) perfusion MRI is based on susceptibility effects using T2-weighted or, more commonly, T2*-weighted images and is the most commonly studied and clinically used perfusion technique in assessment of brain masses and stroke. This method is based on the principle that the signal change that occurs during passage of a high-concentration bolus of gadolinium contrast material in the vessels causes a difference in susceptibility between the vessels that contain contrast material and brain tissue and that this signal change can be converted to a relaxation rate change proportional to the fraction of blood volume within each voxel.3,4 Data generally are acquired during first-pass perfusion over approximately 1 minute, during which time a high-concentration bolus of gadolinium chelate is rapidly injected intravenously. Time-signal intensity curves drawn during this acquisition will show a rapid decline in signal as the contrast enters the brain, with return of the signal to near baseline after the first pass (Fig. 28-1). These measurements are used to construct a relative CBV map, and the time signal intensity curve can be used to derive other perfusion parameters by various mathematical methods.1,5,6 Figure 28-1 Acquisition of dynamic susceptibility contrast perfusion magnetic resonance imaging. To provide adequate temporal resolution during dynamic contrast administration, most centers currently use gradient echo planar imaging sequences to perform clinical DSC perfusion MRI.7–9 This technique is very sensitive to structures that cause magnetic field inhomogeneity such as blood, calcium, bone, metals, or air interfaces such as the skull base. The use of DSC imaging entails multiple technical considerations.10,11 Accuracy of CBV maps can vary substantially depending on the acquisition and postprocessing methods used.6 It is important to take into consideration the type of acquisition used in applying research results for characterization of lesions, because the results and thresholds may vary.12 Derivation of the perfusion parameters also depends on the mathematical models used by the various processing software, and caution must be exercised in comparing results from different calculation methods.13,14 Sometimes a small prebolus dose of contrast material is given before the actual DSC acquisition to correct for leakage and more accurate calculation of the perfusion parameters.6,10 DSC perfusion applications are used predominantly to assess cerebrovascular disease and in brain tumor management (e-Fig. 28-2). DSC perfusion can assess the ischemic penumbra in persons who have had an acute stroke and aid in the imaging triage and management of these patients.15,16 DSC perfusion has been used in differentiation of brain tumors from other masslike lesions in the brain, preoperative grading of brain tumors, differentiation of primary from metastatic tumors, assessment of treatment response, and differentiation of radiation necrosis from a recurrent tumor.1,17–23 e-Figure 28-2 Perfusion magnetic resonance (MR) imaging in a 17-year-old patient with an anaplastic astrocytoma a few months after surgical resection and chemoradiation therapy. ASL perfusion imaging does not require exogenous contrast injection. It uses magnetically labeled arterial blood water as an endogenous flow tracer.24 A general scheme of the ASL technique is illustrated in Figure 28-3. Two sets of images are obtained, one as a baseline image of the brain and the other after labeling (or tagging) blood arterial water protons in the neck using an inversion or saturation radiofrequency pulse. This second set is obtained after a short delay time that allows the labeled blood to flow into the imaging slices. If the baseline and postlabel images are subtracted from each other, the resulting subtracted image is proportional to blood flow that has entered the brain. Quantitative measures of CBF can then be derived from the subtracted images. Numerous schemes exist for ASL tagging and imaging; however, the details are beyond the scope of this chapter.25 Typically, echoplanar or spiral nonechoplanar techniques are used for image acquisition. ASL imaging takes significantly longer than DSC perfusion MRI because the signal change resulting from the arterial spin label is very small (in the order of 0.5% to 3%), and therefore numerous signal averages need to be acquired to gain acceptable signal to noise. Imaging at 3 Tesla significantly increases the signal and quality of ASL images. Given the requirement for image subtraction and longer acquisition times, ASL perfusion is very sensitive to motion artifacts. Figure 28-3 A schematic demonstration of the general principle of arterial spin labeling perfusion magnetic resonance imaging. Applications of ASL perfusion include cerebrovascular disease, detection of changes during complicated migraine (Fig. 28-4), hypoxic-ischemic injury, depiction of hypoperfusion in mesial temporal sclerosis, and emerging applications in brain tumors.26–32 Further work is needed to establish the role of ASL imaging in pediatrics. Figure 28-4 Arterial spin labeling (ASL) in a child with hemiplegic migraine. Dynamic CT perfusion imaging bears some similarity to DSC perfusion MRI in that perfusion parameters are derived from a time-concentration curve obtained during continuous scanning of the first pass of a rapid injection of iodinated contrast material through the brain.1,33,34 Quantitative maps of CBV, CBF, and MTT can be obtained. Dynamic CT perfusion imaging has the advantage of widespread availability and speed, which can be important in the setting of acute stroke or in patients with contraindications to MRI. CT perfusion imaging often is performed in conjunction with CT angiography in the evaluation of cerebrovascular disease. Although continuous scanning of the head for CT perfusion can lead to exposure to a high radiation dose, CT perfusion can be performed satisfactorily with 80 kVp and a low mA technique, which considerably decreases the radiation dose.1,35 CT perfusion imaging has been studied extensively in the evaluation of patients with cerebrovascular disease, especially in the setting of acute ischemic stroke.33,36 It can demonstrate the ischemic penumbra and tissues at risk and can be helpful in patient management (Fig. 28-5).1,33
Perfusion Imaging and Magnetoencephalography
Perfusion Imaging

Perfusion MRI
Dynamic Susceptibility Contrast Perfusion MRI
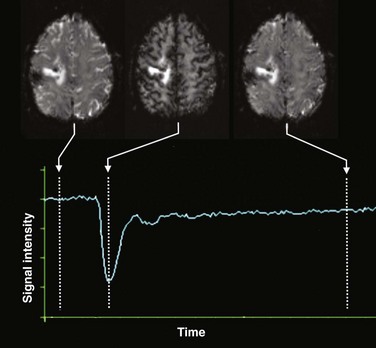
Typically, a rapid echo planar acquisition is obtained through the head continuously over the course of approximately 1 or 1.5 minutes. A rapid injection of gadolinium-based contrast material is injected, which results in a transient dip in the signal intensity during the course of the first pass of contrast through the brain. After this first pass, the signal returns toward normal, although often not completely. A time-signal intensity curve is plotted before, during, and after the first pass bolus for each voxel, including brain tissue and vascular structures, which in turn is used to derive various perfusion parameters.
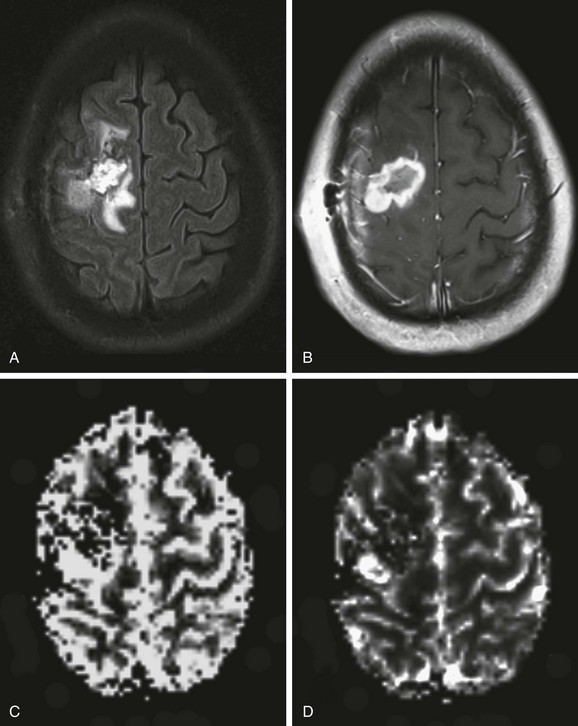
An axial fluid-attenuated inversion recovery image (A) and postcontrast T1-weighted image (B) demonstrate a surgical resection cavity with signal abnormality and enhancement around the cavity. Relative blood volume (C) and blood flow (D) maps derived from dynamic susceptibility contrast MR perfusion demonstrate a focus of abnormally increased perfusion posterolateral to the surgical resection cavity consistent with recurrence and progression of the neoplasm.
Arterial Spin Labeling Perfusion MRI
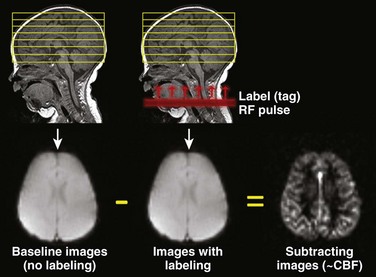
Images of the head are obtained once without and once with labeling of blood water protons using a radiofrequency (RF) pulse. The labeled (or tagged) blood flows into the brain, and if the images without and with label are subtracted from each other, the difference image results from these labeled blood protons and is proportional to cerebral blood flow (CBF).
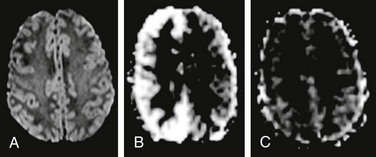
The patient presented with acute onset left-sided weakness in the face and both the upper and lower extremities, along with headache. Magnetic resonance imaging (MRI) was emergently performed to exclude an arterial ischemic stroke. No abnormality was found on diffusion-weighted imaging (A), but ASL perfusion MRI demonstrated increased cerebral blood flow in the right cerebral hemisphere (B). Two days later, the patient’s symptoms have completely resolved and a repeat MRI demonstrated normal appearance of the brain on ASL perfusion imaging (C).
Computed Tomographic Perfusion Imaging
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Perfusion Imaging and Magnetoencephalography





