Term
Term
37 completed weeks to 41 weeks and 6 days
Premature
Preterm
<37 weeks
Low birth weight
LBW
<2,500 g
Very low birth weight
VLBW
<1,500 g
Extreme low birth weight
ELBW
<1,000 g
Small for gestational age
SGA
BW <10th percentile for GA
Large for gestational age
LGA
BW >90th percentile for GA
Absolute neutrophil count
ANC
White cell count x % that are neutrophils
Severe neutropenia
ANC <0.5 × 109/L
Normal urine output
Infants and young children: 1.5–2 mL/kg/h
Older children and adolescents: 1 mL/kg/h
Estimated body weight (in kg) based on child’s age
Children 1–9 years: (age in years × 2) + 8
Children >10 years: age in years × 3.3
Endotracheal tube size (internal diameter in mm)
Infants <1 year: 3.5 mm (uncuffed)
Children 1–2 years: 4 mm (uncuffed)
Children 2–10 years: 4 + (age/4) (uncuffed)
Children 2–10: 3.5 + (age/4) (cuffed)
Hypothermia
Core temperature< 35 °C
ASA 1 | Normal healthy patient |
ASA 2 | A patient with mild systemic disease |
ASA 3 | A patient with severe systemic disease |
ASA 4 | A patient with severe systemic disease that is a constant threat to life |
ASA 5 | A moribund patient who is not expected to survive without the operation |
ASA 6 | A declared brain-dead patient whose organs are being removed for donor purposes |
Prefix “e” | Emergency |
Test name | Age | Reference values |
|---|---|---|
Activated partial thromboplastin time (APTT) | <3 month | 25–35 s |
>3 month | 23–35 s | |
INR | <3 month | 0.9–1.6 |
>3 month | 0.9–1.1 | |
Hemoglobin | <30 days | 140–200 g/L |
1 month | 115–180 g/L | |
2 months | 90–135 g/L | |
3–11 months | 100–140 g/L | |
1–4 years | 110–140 g/L | |
5–13 years | 120–160 g/L | |
≥14 years female | 120–153 g/L | |
≥14 years male | 140–175 g/L | |
Creatinine | ≤6 days | 19–90 μmol/L |
7–60 days | 10–56 μmol/L | |
2 months–5 years | <36 μmol/L | |
6–9 years | <53 μmol/L | |
10–13 years | <79 μmol/L | |
≥14 years | <98 μmol/L | |
Glucose * | <1 year | 2.5–5.5 mmol/L |
1–2 years | 2.5–5.0 mmol/L | |
3–11 years | 2.8–6.1 mmol/L | |
≥12 years | 3.3–6.1 mmol/L |
Table 2.4
Fasting guidelines for GA or sedation (may vary slightly from institution to institution) [8]
Clear fluids | 2 h |
Breast milk | 4 h |
Infant formula/cow’s milk | 6 h |
Solids | 8 h |
Table 2.5
Example “time-out” checklist
All team members to stop what they are doing and take part in time-out |
|---|
• Staff present |
– Operator(s) |
– Anesthesiologist |
– Nurse |
– Technologist |
• Patient name |
• Patient identification |
• Patient diagnosis/history |
• Procedure to be performed |
• Procedures by other services to be performed |
• Written consent |
• Correct site and correct side marked (on patient) |
• Patient allergies |
• Blood work reviewed |
• Last menstrual period/pregnancy test results |
• Prophylactic antibiotics |
• Correct name on imaging equipment |
• Correct orientation on equipment |
• Correct side markers in place on equipment |
• Radiation protection equipment in place |
• Grid in/out |
• Any potential adverse events expected |
• Equipment for adverse events inside/outside of room |
– Crash cart |
– Blood warmer |
– Blood products |
– Warming lights/blankets for neonates |
• Equipment for procedure in room |
• Any other concerns or comments from any team member in room? |
Age | Weight (kg) (approx) | HR awake | HR sleeping | RR | BP | ETT size |
|---|---|---|---|---|---|---|
Birth | 3.5 | 85–205 | 80–160 | 30–60 | 65/40 | 3.0–3.5 |
6 months | 7.5 | 110–160 | 80–160 | 24–38 | 85/50 | 3.5–4.0 |
1 year | 10 | 90–150 | 75–160 | 22–30 | 90/55 | 4.0 |
3 years | 14 | 80–125 | 60–90 | 22–30 | 92/55 | 4.5 |
5 years | 18 | 70–115 | 60–90 | 20–24 | 95/58 | 5.0–5.5 |
10 years | 30–32 | 60–100 | 50–90 | 16–22 | 100/62 | 6.0–6.5 |
12 years | 40 | 60–100 | 50–90 | 16–22 | 106/62 | 6.5 |
14 years | 45 | 60–100 | 50–90 | 14–20 | 110/66 | 6.5–7.0 |
Age | Pulse rate/min | Blood pressure (systolic) | Respiratory rate/min |
|---|---|---|---|
≤3 months | <80 or >200 | <60 mmHg | <30 or >60 |
3–12 months | <80 or >180 | <65 mmHg | <24 or >50 |
1–10 years | <60 or >150 | <70 + (2 × age in years) | <22 or >40 |
• 10 years | <60 or >120 | <90 mmHg | <12 or >30 |
Table 2.8
Commonly used drugs (in alphabetical order)
Name | Dose |
|---|---|
Acetaminophen | 15 mg/kg PO |
Adenosine | 0.1 mg/kg/dose IV rapidly |
Cefazolin | 30 mg/kg/dose IV |
Cefoxitin | 30 mg/kg/dose IV |
Diphenhydramine | 1–2 mg/kg/dose IV (anaphylaxis) |
Fentanyl | 1 μg/kg/dose IV |
Flumazenil | 10 μg/kg IV over 15 s. Wait 1–3 min. Repeat up to four times |
Glucagon | 0.02–0.03 mg/kg/dose. Max dose 0.5 mg <20 kg; 1 mg > 20 kg |
Heparin | 50–100 units/kg to max 5,000 units loading dose |
Ketamine | 0.25 mg/kg/dose IV |
Midazolam | 0.05 mg/kg/dose IV; 0.5 mg/kg/dose PO <20 kg; 0.3 mg/kg/dose >20 kg |
Morphine | 0.05 mg/kg IV dose |
Naloxone | 0.001–0.01 mg/kg/dose for narcotic reversal in sedated patients |
Sucrose | 23–32 weeks: up to 0.5 mL PO 2 min prior to procedure |
32–37 weeks: up to 1 mL PO 2 min prior to procedure | |
>37 weeks: up to 2 mL PO 2 min prior to procedure | |
All infants who are NPO: up to 0.5 mL PO 2 min prior to procedure. Dose may be administered in increments of 2-min intervals for prolonged procedures; divided or repeated to the maximum daily dose. Maximum daily dose: four times in 24 h | |
Topical anesthetic | Lidocaine (Maxilene) topical anesthetic cream: 2 %—thin layer to skin |
Tetracaine (Ametop) 4 % cream/patch—thin layer to skin |
Table 2.9
IV Fluid maintenance and bolus guidelines
Maintenance | ||
|---|---|---|
Weight | Daily volume | Hourly volume |
1–10 kg | 100 mL/kg/day | 4 mL/kg/h |
11–20 kg | 50 mL/kg/day | 2 mL/kg/h |
>20 kg | 20 mL/kg/day | 1 mL/kg/h |
Bolus | ||
Hypovolemic shock | 20 mL/kg bolus, repeat prn | Give rapidly over 5–10 min |
Cardiogenic shock | 5–10 mL/kg bolus, repeat prn | Give slowly over 10–20 min |
Table 2.10
Sodium recommended in routine post-procedure fluids
Fluid | Na+ mmol/L | K+ mmol/L | Dextrose g/100 mL | Tonicity |
|---|---|---|---|---|
D5W (dextrose 5 % in water) | 0 | 0 | 5 | Hypotonic |
D10W (dextrose 10 % in water) | 0 | 0 | 10 | Hypotonic |
NS (normal saline, 0.9 % NaCl) | 154 | 0 | 0 | Isotonic |
½ NS (half normal saline, 0.45 % NaCl) | 77 | 0 | 0 | Half-isotonic |
 | 45 | 0 | 3.33 | Hypotonic |
Ringers lactate | 130 | 4 | 0 | Isotonic |
As outlined in Chap. 1, it is no longer standard of care for interventional radiology (IR) physicians to perform procedures and leave the entire care of the patient to their referring team [1–4]. Increasingly IRs are actively involved in the continuum of patient care, following their patients pre- and post-procedure, either in the capacity of a consulting service or assuming full responsibility with admitting privileges. Many IRs without admitting privileges are actively seeking to obtain such privileges.
Details of specific procedures are dealt with in individual chapters. This chapter will address the following general aspects of periprocedural care:
(a)
Pre-procedure clinical care
(b)
Clinical care during the procedure
(c)
Post-procedure care
Pre-procedure Clinical Care
Patient Assessment
The requirement for pre-procedure assessment depends on the nature of the procedure to be undertaken and ranges from minimal (such as for a gastrostomy tube check) to full IR pre-procedure evaluation, as in a patient with complex vascular malformation seen in a multidisciplinary clinic (see Chap. 1). Much of the IR workload can be considered “service work,” in which case IR provides a valuable supportive service for a large number of patients referred from a variety of specialties, for example, when providing central venous access for surgical and oncologic patients. In other instances, IR provides the definitive therapeutic procedure for a variety of conditions, such as embolization of an arteriovenous malformation. Irrespective of the type of procedure considered, clearly it is important to ensure that the IR procedure requested is indicated and appropriate for that individual patient and to weigh the risk factors or contraindications prior to undertaking the procedure. Making this assessment may necessitate an IR clinic or multidisciplinary clinic visit. At such a visit, a clinical history is taken, physical examination is performed, necessary imaging is reviewed, and any required specialty consultation, imaging, or blood work is organized.
Evaluation of Imaging
Careful evaluation of available imaging is important in order to confirm that the procedure, for example, a biopsy or abscess drainage, is technically possible and clinically appropriate. If there is any uncertainty about access, choice of modality to be used, or suitability for the planned procedure, this can be resolved by pre-procedure “mapping” imaging, ideally performed by an interventionalist, with the very specific and focused questions below in mind (different than those asked in a standard diagnostic imaging exam):
(a)
Is the lesion well visualized with this imaging modality, or is another modality required?
(b)
Can the lesion be safely accessed percutaneously, avoiding interposed vessels and other relevant structures, such as bowel or pleura?
(c)
What are the risks and benefits of different trajectories or angles?
(d)
What level of sedation/anesthesia is required for this patient for this procedure?
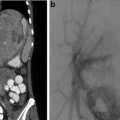
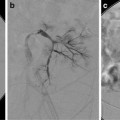
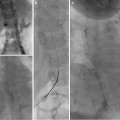
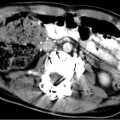
Mapping imaging may involve ultrasound, fluoroscopy, CT, or a combination of imaging modalities (e.g., combination of US and fluoroscopy mapping to assess the feasibility of placing a gastrostomy tube in an infant with distorted abdominal anatomy post diaphragmatic hernia repair). Mapping will determine the imaging required (e.g., should US or CT be used to access a small peripheral pulmonary nodule for biopsy) [5]. Time taken for pre-procedural mapping is time well spent, as it improves the accuracy of procedure planning, decreases the need for last-minute changes to the plan, enables the case to be scheduled with the most suitable equipment (e.g., CT scanner if needed), and avoids the situation where the patient must be moved during a case or, even, the procedure canceled. In addition, an appointment for mapping gives the parents and child an opportunity to visit the IR department and meet members of the team. The results of the mapping imaging are shared with the referring physician and the family, and a plan to proceed (or not proceed) is reached. This visit also provides an opportunity to obtain informed consent well in advance of the procedure, which is preferable to obtaining written consent immediately prior to the procedure, as the more relaxed setting allows a more adequate consent process for the family.
Consultations
Specialty consultation may need to be arranged prior to a procedure. Most commonly this involves an anesthesia consultation, usually indicated in children with known airway difficulties, complex cardiopulmonary problems, or American Society of Anesthesiology (ASA) Class 4 or 5 (Table 2.2) [6]. Additional investigations if required by the anesthesiologist are arranged in advance of the procedure (e.g., in an acute setting, an ECG, cardiology consultation, and echocardiography in a patient with a large anterior mediastinal mass pre-biopsy to evaluate pulmonary artery and venous flows, vascular compression, as well as the cardiac ejection fraction) [7]. Other examples include an ophthalmology consultation to evaluate eyes/vision prior to management of a periorbital vascular malformation or a cardiology consult in a child with cardiac symptoms or signs.
Blood Analyses
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


