• Direct communication with clinical team is essential
DIAGNOSTIC CHECKLIST
• Important to recognize pneumatosis intestinalis, but significance depends on etiology and clinical setting
• Nonischemic causes of pneumatosis are usually asymptomatic, of little clinical significance
• Recognition of pneumatosis demands direct communication with clinical team to determine its likely etiology and optimal management
(Left) CT in a 50-year-old man on chronic steroid medication for psoriasis shows gas within the colon wall , but the colon and SB show normal caliber. Note the free intraperitoneal gas . This was a persistent asymptomatic finding attributed to medication.
(Right) CT shows extensive pneumatosis throughout the SB. Bowel distention and ascites help to confirm that the pneumatosis is likely on the basis of bowel ischemia, rather than one of the “benign” (nonischemic) causes of pneumatosis.
(Left) Axial CECT in a 75-year-old man who presented with abdominal pain and prior bowel ischemia demonstrates relatively subtle gas within the peripheral intrahepatic branches of the portal vein .
(Right) Axial CECT in the same patient reveals extensive pneumatosis within dilated segments of the bowel. Ascites is also noted near the damaged bowel. The patient went to surgery for resection of the infarcted bowel.
TERMINOLOGY
Synonyms
Definitions
• Cystic or linear collections of gas in subserosal or submucosal layers of gastrointestinal (GI) tract wall
• Pneumatosis intestinalis: Most common form of intramural gas, found in small bowel more often than colon
• Pneumatosis coli: Rounded collections of gas in distal colonic wall, usually asymptomatic finding
• Pneumatosis is a descriptive sign, not a disease or diagnosis
IMAGING
General Features
• Best diagnostic clue
Cystic or linear distribution of gas along bowel wall on CT
Radiographic Findings
• Radiography
Fluoroscopic Findings
• Barium studies
Pneumatosis intestinalis
– Mottled, bubbly, or linear collections of gas in bowel wall; feces-like appearance
– Dilated bowel loops ± thumbprinting
Pneumatosis coli
– Radiolucent cysts resembling polyps, clustered along colonic contours
– Multiple large gas-filled cysts with scalloped defects in bowel wall, mimicking inflammatory pseudopolyps
– Concentric compression of colonic lumen by cysts
– Striking lucency of gas-filled cysts
CT Findings
• CECT
Pneumatosis intestinalis
– Band-like: Bands or linear distribution of gas in affected bowel wall




 , but the colon and SB show normal caliber. Note the free intraperitoneal gas
, but the colon and SB show normal caliber. Note the free intraperitoneal gas  . This was a persistent asymptomatic finding attributed to medication.
. This was a persistent asymptomatic finding attributed to medication.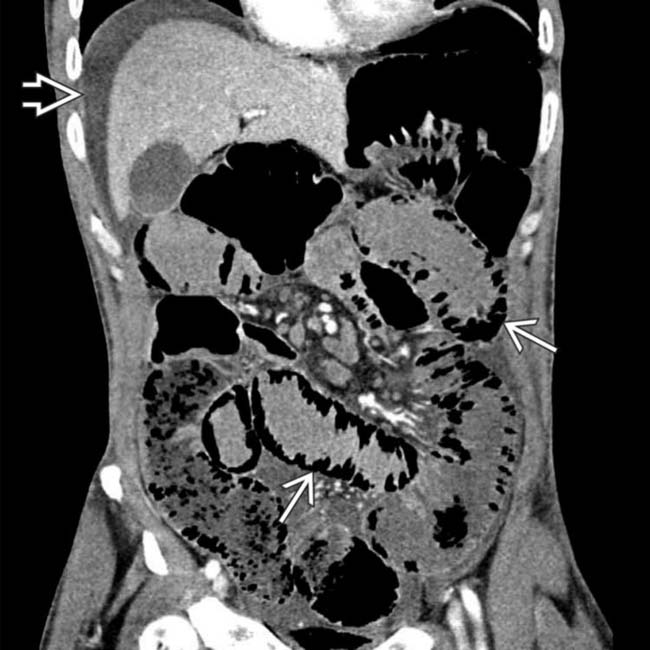
 throughout the SB. Bowel distention and ascites
throughout the SB. Bowel distention and ascites  help to confirm that the pneumatosis is likely on the basis of bowel ischemia, rather than one of the “benign” (nonischemic) causes of pneumatosis.
help to confirm that the pneumatosis is likely on the basis of bowel ischemia, rather than one of the “benign” (nonischemic) causes of pneumatosis.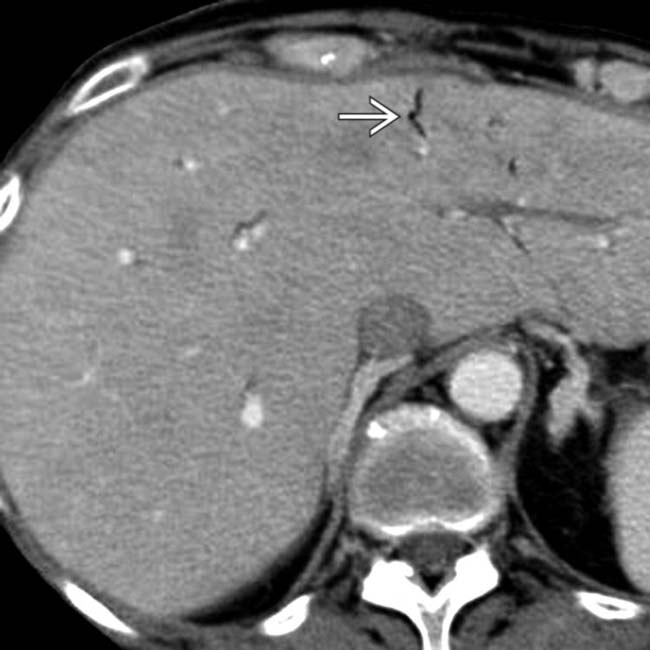
 .
.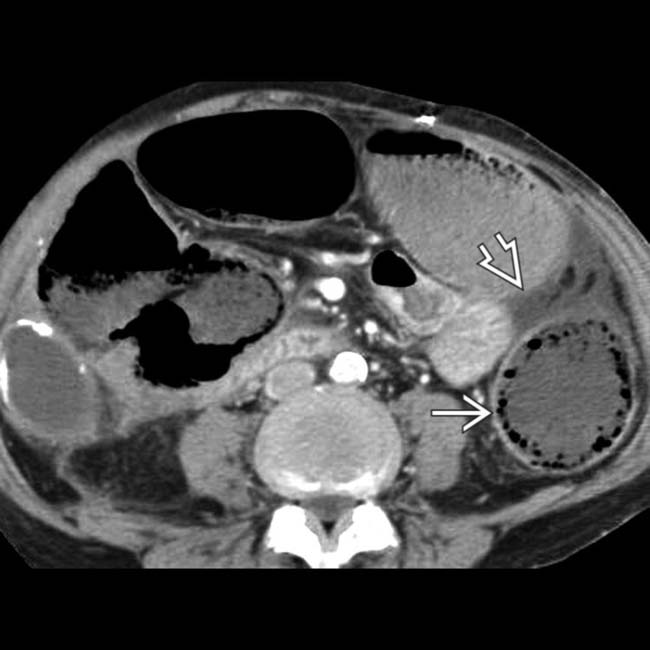
 within dilated segments of the bowel. Ascites is also noted
within dilated segments of the bowel. Ascites is also noted  near the damaged bowel. The patient went to surgery for resection of the infarcted bowel.
near the damaged bowel. The patient went to surgery for resection of the infarcted bowel.





















