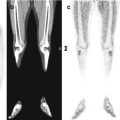
Fig. 14.1
(a–d) The patient underwent PET/CT, which showed hypermetabolic soft tissue at the tracheostomy site. This was more likely an infectious/inflammatory change than malignancy. Otherwise, there were no suspicious hypermetabolic lesions
She received radioimmunotherapy (131I, activity: 155.23 mCi). The post-therapy 131I scan did not show uptake in the lateral neck, lungs, or bones. The synthroid dose was adjusted to keep TSH suppressed to close to 0.1 ng/ml.
After 4 months, the patient developed two masses in the left neck, which on MRI measured 5 × 3.8 and 3.0 × 2.3 cm (Fig. 14.2). Thyroglobulin increased until 27 ng/ml.
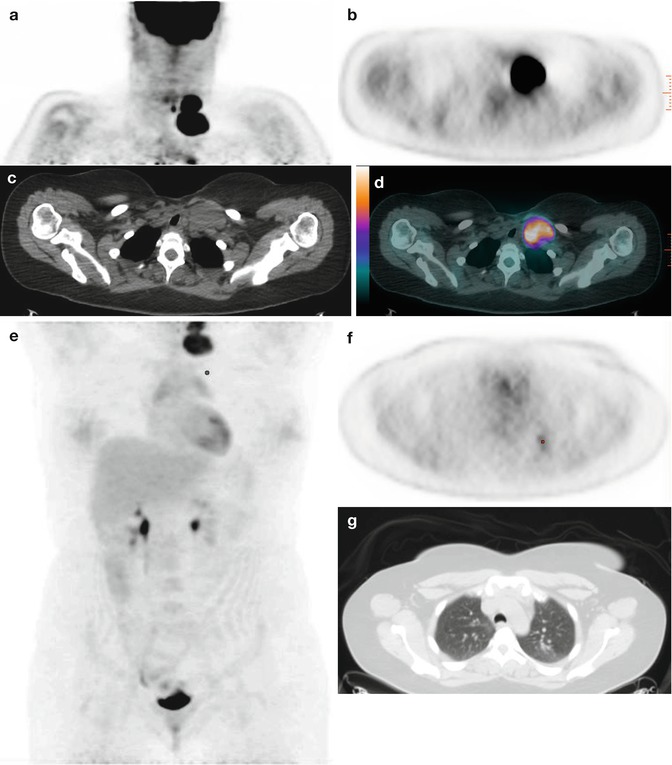
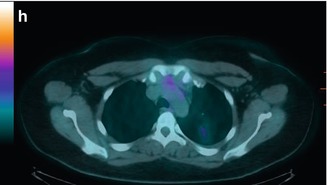
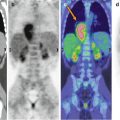
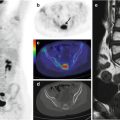
Fig. 14.2




(a–d) The PET/CT study showed a new, hypermetabolic bilobed mass in the left neck that was suspicious for relapse malignancy (SUVmax 12.0) and (e–h) mild FDG uptake associated with a left upper lobe nodule seen on CT, possibly malignancy or inflammatory change
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
