Positron Emission Tomography/Computed Tomography and Biologically Conformal Radiation Therapy
Positron Emission Tomography/Computed Tomography and Biologically Conformal Radiation Therapy
Marco Trovo
Jeffrey Bradley
Mitchell Machtay
Positron emission tomography (PET) is a noninvasive imaging technique that exploits the unique decay physics of positron-emitting isotopes. The isotopes of fluorine have been used in the development of diagnostically useful biologic compounds that are available for PET imaging in order to provide a metabolic assessment of normal tissue or disease conditions. [18F]Fluorodeoxyglucose ([18F]FDG), as PET tracer, is now being used in the evaluation of several neoplasms, both before and after treatment, as well as in the planning of radiation therapy in various cancers. The method is based on identifying the increased glycolytic activity in malignant cells, in which glucose is preferentially concentrated due to an increase in membrane glucose transporters as well as to an increase in some of the principal enzymes, such as hexokinase, responsible for phosphorylation of glucose. 2-(Fluorine-18)fluoro-2-deoxy-D-glucose (FDG) is transported into tumor cells, similarly to glucose, by means of glucose transporter proteins known as GLUT transporters and subsequently phosphorylated by hexokinase to FDG 6-phosphate. FDG 6-phosphate is not efficiently metabolized further and therefore accumulates within cell. This process of “metabolic trapping” of FDG in the cell constitutes the basis for imaging of the in vivo distribution of the tracer with FDG-PET.
NON-SMALL-CELL LUNG CANCER
T STAGE
According to a recent meta-analysis published by Gould, the sensitivity of FDG-PET for detecting lung carcinomas ranges from 83% to 100%, whereas the specificity is extremely variable.1 The mean sensitivity and specificity were found to be 96.0% and 73.5%, respectively. Therefore, it can be asserted that FDG-PET is an accurate test for the identification and characterization of malignant pulmonary lesions, and this exam should be included in the assessment of malignancy of suspicious lung nodules. However, inherent limitations of PET include its failure to depict anatomic landmarks and its limited spatial resolution, which restrict its use for assessing tumor size and potential infiltration of the thoracic wall, mediastinum, or other adjacent structures. Therefore, FDG-PET is not recommended for determination of tumor T stage (size or invasion of adjacent structures) but, instead, for determining the malignant potential of lung lesions.
Although [18F]FDG is an exquisite tumor-localizing tracer, it is not tumor specific. The uptake of [18F]FDG reflects glucose metabolism in essentially any issue. Its increased uptake in tumors is a result of increased and inefficient use of glucose. Other benign processes associated with cells that have increased glucose use, such as inflammation, also have enhanced [18F]FDG uptake. In the assessment for lung cancer, granulomas that occur in patients with sarcoidosis, tuberculosis, histoplasmosis, aspergillosis, coccidioidomycosis, and other infectious processes such as pneumonia may result in false-positive findings. Tumors with low metabolic activity such as carcinoid tumors and bronchoalveolar cell carcinomas may not demonstrate significant tracer uptake. Occasionally, well-differentiated adenocarcinomas have relatively less intense FDG accumulation, particularly lesions <1.0 cm in diameter. Recognition of these imaging pitfalls with [18F]FDG is essential in the staging of patients before treatment.
N STAGE
FDG-PET has been successfully used in the evaluation of mediastinal lymph nodes and in the detection of distant metastases. Mediastinal lymph node involvement and distant metastases significantly affect the prognosis of non-small-cell lung cancer (NSCLC), making accurate staging crucial for the selection of appropriate treatment. Although computed tomography (CT) provides significant anatomic information regarding the extent of intrathoracic tumor, this technique has limited accuracy in the detection of hilar or mediastinal lymph node metastases. The reported CT sensitivity, specificity, and accuracy in detecting mediastinal node metastases have been extremely variable.2, 3, 4, 5, 6, 7, 8, 9, 10, 11 False-positive rates have varied from 20% to 45%, and false-negative rates have varied from 7% to 39%. Thus, a more accurate method to delineate the extent of spread of tumor progression in NSCLC is essential for both the staging and the subsequent treatment planning process. Thus, radiation treatment planning based only on CT findings is likely to lead to geographic miss of regions of macroscopic tumor in some patients and lead to the irradiation of unnecessarily large volumes in others.
PET has consistently been shown to be more accurate than CT12 in the evaluation of mediastinum in patients with NSCLC. In one of the largest studies, Pieterman et al.13 evaluated 102 patients with resectable NSCLC and compared the results of PET and CT. The sensitivity and specificity of PET for detection of mediastinal metastases were 91% and 86%, respectively. The corresponding values for CT were 75% and 66%, respectively (p <0.001). The overall negative predictive value (NPV) of PET was 95%, and positive predictive value (PPV) was 74%. PET produced false-positive results in seven patients because of the presence of reactive hyperplasia and in three patients because of silicoanthracosis. False-negative results were due to microscopic tumor residue in two patients and to the inability of the method to distinguish between paramediastinal primary tumor and mediastinal lymph nodes in one patient. Moreover, PET identified distant metastases not detected by standard methods in 11 of the 102 patients. The use of PET resulted in lowering of the clinical stage in 20 patients and upstaging in 42 patients. Thus, it is predictable that combination of PET with CT will provide an improvement over CT alone for targeting radiation therapy. Similar results were reported by Gupta et al.14 Results of FDG-PET and CT were compared for detecting mediastinal nodal disease and distant disease in 71 patients with lung cancer considered candidates for surgical resection. PET was significantly more sensitive than CT in detecting N2 or N3 disease. The sensitivity, specificity, and accuracy of PET in detecting metastatic disease in lymph nodes were 93%, 94%, and 96%, respectively. The efficacy of PET was significantly superior to that of CT, which had a sensitivity, specificity, and accuracy of 63%, 60%, and 61%, respectively. PET changed N staging in 35% of patients. Lymph node staging was advanced in 14 patients and downstaged in 24 patients. The superiority of PET imaging over CT in detecting metastatic involvement of lymph nodes has also reported in several other studies.12,15,16
A meta-analysis published by Dwamena et al.17 compared the ability of PET versus CT to stage the mediastinum. The authors analyzed the staging performance of PET in 14 studies that included 514 patients and CT in 29 studies that included 2,226 patients. From summary receiver operating characteristic (ROC) curves and pooled point estimates of diagnostic performance, FDG-PET was found to be significantly more accurate than CT for identifying nodal metastases. The mean sensitivity and specificity were 70% and 91%, respectively, for PET and 60% and 77%, respectively, for CT. A more recent meta-analysis by Toloza et al.18 compared the results of CT and PET in staging of mediastinal nodes. Twenty studies with more than 3,400 assessable patients evaluated the accuracy of standard CT for staging of the mediastinum, and 18 studies, which included >1,000 assessable patients, assessed the value of PET. The pooled sensitivities were 57% and 84% for CT and PET, respectively; the pooled specificities were 82% and 89%, respectively. The authors revealed that there was a marked heterogeneity in the sensitivity and specificity of CT studies, whereas the heterogeneity of PET studies was much less relevant. The overall PPV and NPV of CT scanning for patients were 56% and 83%, respectively, and the overall PPV and NPV for PET were 79% and 93%, respectively. This recent meta-analysis demonstrates that the accuracy of CT scanning for mediastinal staging has not improved over the past decade, despite the improvement in CT scan resolution. Thus, FDG-PET in combination with CT may be superior to CT alone for targeting hilar or mediastinal lymph nodes involved with cancer.
M STAGE
FDG-PET also has an advantage over the combination of other routine studies required to determine the M stage. Forty percent of patients with newly diagnosed lung cancer have distant metastases at presentation, although clinical and laboratory indicators for metastases are nonspecific, with an accuracy of only 50%.19,20 Marom et al.21 compared the accuracies of FDG-PET and conventional imaging (thoracic CT, bone scintigraphy, and brain CT or magnetic resonance imaging [MRI]) in 100 patients with newly diagnosed bronchogenic carcinoma. PET staging was accurate in 83% of patients, whereas conventional imaging was accurate in 65% of patients. Overall, PET showed greater accuracy than conventional imaging in the detection of distant metastases. PET identified unsuspected distant metastases in 9% of patients that were not found with conventional imaging. PET was 92% sensitive and 99% specific for bone metastases, whereas bone scintigraphy had 50% sensitivity and 92% specificity. Thus, the whole-body FDG-PET study can eliminate the need for staging bone scintigraphy.
Approximately two thirds of adrenal masses detected with conventional imaging in patients with lung cancer are reported to be benign. This low PPV often leads to an unnecessary adrenal biopsy. In the study reported by Marom et al.,21 the PPV of FDG-PET for adrenal metastases was 100%.
The normal brain has substantial glucose uptake, and a focal area of abnormal accumulation in the brain due to metastases may be difficult to detect with FDG-PET. The low sensitivity (60%) is problematic; thus, FDG-PET is not a replacement for brain MRI or CT imaging.
van Tinteren et al.22 reported a randomized prospective trial in patients with suspected NSCLC who were scheduled for surgery after conventional workup to test whether FDG-PET reduced the number of futile thoracotomies. Only patients with stage I/II disease were enrolled. FDG-PET confirmed distant disease in 8% of patients who underwent PET, in addition to conventional staging, whereas distant metastasis was detected in only 2%. These data are in line with other studies, where unexpected distant metastases have been reported in up to 14% of patients.14
RADIATION TREATMENT PLANNING
The incorporation of FDG-PET information into radiation therapy planning is very common today. Incorporation of PET into the treatment planning process has the potential to make determination of the gross tumor volume (GTV) much more accurate and thus reduce the risk of futile therapy. When clinical PET first became available to oncologists, there were no readily available means for incorporating PET information directly into the treatment planning process. Typically, PET and diagnostic CT images were simply displayed side by side, and the radiation oncologist would visually incorporate the PET information when contouring the GTV. This method is suitable for small anatomically discrete structures that are easily seen on CT, but it is not an optimal method for helping to delineate the boundaries of larger tumors where the margins are not well imaged on CT, such as the interface between a lung tumor and atelectasis. For that purpose, it is necessary to display PET and CT information simultaneously within the treatment planning software.
When the PET and CT scans are obtained on separate units, systems have been developed that use fiducial markers to help with accurate image fusion. Prior to the installation of the PET/CT scanner at our center, patients were positioned identically by radiation therapists in the treatment position, using lasers installed in both the CT and PET suites. PET images and CT images were then fused by commercial software, using the fiducial markers.
The optimum data set for radiotherapy planning is provided by a modern combined PET/CT scanner. PET and CT images are acquired on the same gantry, without the need of repositioning the patient. Modern treatment planning systems, such as Focalease (Computerized Medical Systems, Inc., St. Louis, Mo) Pinnacle (Philips Medical Systems, Eindhoven, the Netherlands) and others, allow seamless transfer of PET/CT data into the contouring workstation and provide a wide range of options for display of fused PET and CT images.
The definition of target volumes by the treating physicians has been found to bear the largest source of error within the chain of planning and delivering radiotherapy.23 The increased use of FDG-PET in the definition of target volumes could reduce this source of error, but an area of controversy surrounding PET/CT planning pertains to the modality with which the PET-defined contours should be obtained. There has been little guidance from the literature on how best to use PET/CT information in contouring tumor and target volumes. There can be major difficulty in determining the boundaries of some tumors that do not have clearly delineated margins on CT component of PET/CT. This is due to the relatively low resolution of the PET part of the image and consequent blurriness of the edge of many structures visualized on PET scans. Motion of patients on the couch and internal motion, such as that related to respiration, also contribute to the blurriness of PET images. Other confounding factors may include regions of low avidity in the tumor due to necrosis and poor contrast between tumors with a low standardized uptake value (SUV) and adjacent normal structures. Whereas CT information is acquired almost instantaneously and represents a snapshot in time, PET information is acquired over many respiratory and cardiac cycles and therefore represents an “average” position of the structures imaged.
There are three main approaches to contouring the edges of tumor on PET/CT. The first is to use a visual interpretation of the PET scan. The definition of the contours of the GTV is only performed after consultation with the nuclear medicine physician who is asked to draw around the edge of the tumor. This visual method can suffer from unacceptable variability due to human factors and is very much dependent on the individual investigator and display window setting. A second approach makes use of the quantitative information available from PET. This method attempts to find a threshold for image segmentation. The SUV is a commonly used parameter for semiquantitative evaluation of tracer uptake in tumors. In diagnostic studies, a maximum SUV of 2.5 is often defined and still discussed as a threshold for the distinction between malignant and benign lesions. A third method uses edge detection methods to delineate the PET-identified tumor in contrast to background activity.
Nestle et al.24 compared the GTVs resulting from four methods in 25 patients with NSCLC. Sets of four GTVs were generated for each case by the following four methods: visually (GTVvis); applying a threshold of 40% (GTV40); using an isocontour of SUV 2.5 (GTV2.5); and using an algorithm, which, determined by phantom measurements, rendered the best fit comparing PET with CT volumes using tumor and background intensities in the planning system (GTVbg). The authors found substantial differences between the four methods of up to 41% in the GTVvis. Overall, GTVvis, GTV2.5, and GTVbg correlated well with the CT-derived GTV, whereas the GTV40 appeared unsuitable for target volume delineation. These findings are in line with the data by Erdi et al.,25 who used the threshold of 40% of maximum SUV (SUVmax) for tumor delineation.
Biehl et al.26 have challenged the hypothesis that GTV segmentation for NSCLC can be carried out using a single SUV threshold. A PET/CT data set of 20 patients with peripheral NSCLC was reviewed. The PET-GTV to CT-GTV ratios were compared at various thresholds, and a ratio of 1 was considered the optimal threshold. The authors found that, overall, the optimal threshold for the best match between the two imaging modalities was 24% ± 9% of the SUVmax. The optimal threshold was associated with the tumor size. It was 15% ± 6% for tumors measuring >5 cm, 24% ± 9% for tumors measuring 3 to 5 cm, and 42% ± 2% for tumors measuring <3 cm. The authors also found that the PET-GTV at the 40% and 20% thresholds underestimated the CT-GTV for 16 of 20 and 14 of 20 lesions, respectively. They concluded that no single threshold delineating the PET-GTV provides an accurate volume definition for all patients.
One of the main reasons why a single threshold model for NSCLC is less than ideal is that it fails to account for the lack of uniformity in FDG uptake due to conditions such as necrosis and hypoxia, which are more likely to occur in larger lesions. The lack of uniformity in the methods with which PET information has been used to delineate tumor contours in the published literature makes it difficult to indicate general guidelines as to how PET information should be optimally used to contour the GTV. Certainly, at the present, there is no method for automatic delineation of the GTV based on FDG uptake. Therefore, although more robust algorithms of GTV segmentation based on PET data are being developed and tested clinically, the radiation oncologist should incorporate PET information in the treatment planning process of NSCLC following visual criteria and rely on the cooperation of an experienced nuclear medicine specialist. A current cooperative group trial within the RTOG (RTOG 0515) compares the impact of FDG-PET on target delineation for NSCLC. Because of the thresholding problems discussed earlier, this trial asks investigators to contour the GTV based on the CT images, using FDG-PET as a guide to decide which nodes are or are not malignant. In the setting of atelectasis, investigators are asked to contour the FDG-avid portions of the collapsed lung via consultation with their nuclear medicine radiologist.
STUDIES OF FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY IN RADIOTHERAPY PLANNING
The studies showing the impact of FDG-PET on radiation treatment planning for lung cancer are shown in Table 9.1. Examples of patients whose radiation treatment plans were altered by FDG PET are shown in Figures 9.1 and 9.2. Several studies reported a significant alteration in tumor volume coverage in approximately 30% to 60% of patients with NSCLC whose treatment was planned using FDG-PET images. In most of these studies, the additional information provided by PET has been incorporated through side-by-side comparison of CT and PET images or by digital overlays of separately obtained PET and CT data (image fusion). In a retrospective study, Nestle et al.27 reported that incorporation of PET findings would have altered the shape of the radiation portals in 12 (35%) of 34 patients. Kiffer et al.28 used a method of graphical coregistration of coronal PET reconstructions overlaid on fluoroscopic simulation films. They found inadequate coverage of the tumor delineation on PET in 4 of 15 patients for whom treatment was planned with CT alone. They also reported an improved demarcation of tumors by PET in three additional patients with atelectasis. Use of the PET images for planning would have altered the radiation therapy portals in 7 (47%) of 15 patients. Vanuytsel et al.29 reported a theoretic comparison of GTV defined by CT with GTV defined by coregistered PET+CT. The pathologic extent of nodal disease was mapped by cervical mediastinoscopy in all patients. CT-based and PET+CT-based nodal maps were compared. PET findings altered the theoretical portals in 45 (62%) of 73 patients. Munley et al.,30 using a software fusion, recorded that 35% of 35 patients had an increase in radiotherapy volumes as a result of PET. Brianzoni et al.31 reported that GTV/clinical target volume (CTV) was increased in 44% and reduced in 6% of 24 lung cancer patients planned using a dedicated PET/CT scanner.
TABLE 9.1 Impact of FDG-PET on Radiation Planning in Patients with NSCLC
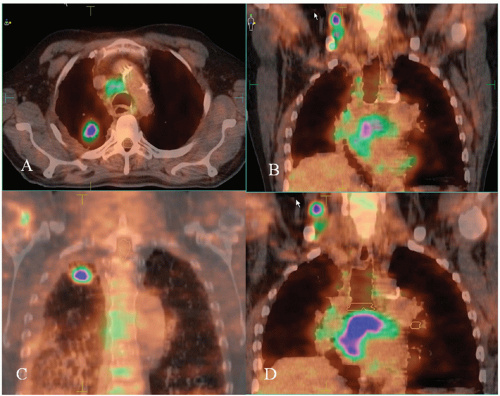
Figure 9.1. Treatment planning positron emission tomography (PET)/computed tomography (CT) shows a right cervical lymph node that was not suspected on physical examination or diagnostic CT imaging. Fine-needle aspiration of the cervical node confirmed adenocarcinoma, consistent with the biopsy from the lung lesion.
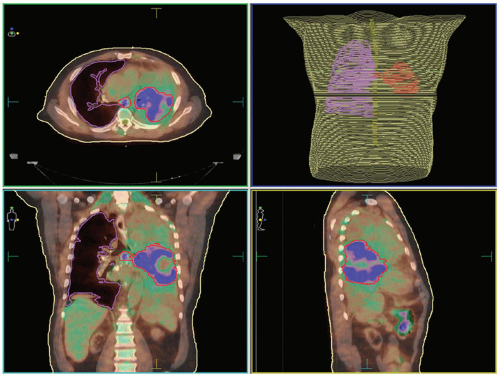
Figure 9.2. Positron emission tomography (PET)/computed tomography (CT) is helpful in the situation of lung atelectasis. In this patient, the PET/CT delineates the tumor mass in the left lung as well as the subcarinal lymph node.
Kalff et al.32 reported that FDG-PET changed or influenced therapy planning for 70 (67%) of 105 patients. Twelve percent of patients were downstaged, and 36% were upstaged, including 14 patients who were found to have metastatic disease. Due to downstaging, three of six patients initially thought suitable only for palliative treatment were recommended for treatment with curative intent. PET prevented aggressive therapy in 27 (35%) of 78 patients initially planned for treatment with curative intent by identifying more advanced disease than previously suspected. In addition, in their prospective study, PET influenced the radiation delivery in 22 (65%) of 34 patients who subsequently received radical radiotherapy treatment volume.
MacManus et al.33 reported on a prospective trial in which diagnostic PET studies were used for radiation therapy planning. Among the 102 patients who underwent definitive irradiation, PET led to a significant increase in the target volume in 22 patients because of the inclusion of structures previously considered not involved by tumor. In 16 patients, the target volume was significantly reduced because PET demonstrated areas of lung consolidation or enlarged lymph nodes with low FDG uptake that were excluded from the treatment volume. Primary tumors were seen on PET in three patients that were not identified on CT. In total, 30% of the locally advanced NSCLC population became ineligible for curative radiotherapy because of either metastatic disease or intrathoracic disease that was too extensive for radical radiation.
A few studies have used radiation therapy simulation based on fusion of CT and FDG-PET. Mah et al.34 performed radiation therapy planning via coregistration of FDG and CT images in 30 patients undergoing definitive radiation therapy for NSCLC. Patients in this prospective study were immobilized for radiation therapy simulation and imaged using a gamma camera. Treatment was significantly altered in 12 patients (40%). The treatment intent became palliative in seven patients. The target volume was altered to include nodal disease detected by coincidence imaging in five patients. The treatment volumes based on CT were judged to be inadequate in comparison with those based on combined CT and FDG-PET imaging in 17% to 29% of patients, depending on the physician who contoured the volumes.
Giraud et al.35 used gamma camera coincidence imaging of FDG fused with simulation CT images using external fiducial markers. Significant alterations in treatment were seen for 5 (45%) of the 11 patients. Additional nodal disease was detected in four patients, and metastatic disease was detected in one patient. Erdi et al.25 reported on 11 patients with NSCLC studied with a dedicated PET scanner who underwent sequential CT and PET simulations. The CT and PET images were then registered in the treatment planning system, and the planning target volume (PTV) was modified on the basis of PET information. There was a change in PTV outline for all patients. The PTV increased in 7 (64%) of 11 patients to incorporate additional regional nodal disease. PET also helped to differentiate tumor from atelectasis in two patients.
Bradley et al.36 prospectively evaluated 26 patients with stage I to III NSCLC referred for definitive radiation therapy or chemoradiation therapy. All patients underwent CT simulation for radiation therapy followed immediately by FDG-PET imaging on a separate scanner. External fiducial markers were used to fuse the two image data sets for radiation therapy planning. The CT alone and PET/CT coregistered images for each patient were maintained separately. The target volume contours were delineated by separate radiation oncologists and compared. FDG-PET findings altered the American Joint Committee on Cancer tumor-node-metastasis (TNM) stage in 8 (31%) of 26 patients, and two patients who were diagnosed with metastatic disease on FDG-PET received palliative treatment. Of the 24 patients whose treatment was planned using three-dimensional conformal radiation therapy, PET significantly altered the radiation therapy volume outlined in 14 patients (58%). PET helped to distinguish tumor from atelectasis in three patients. Unexpected nodal disease was detected by PET in 10 patients. A separate tumor focus within the same lobe of the lung was detected in one patient.
In a large retrospective study comprising 101 patients with NSCLC eligible for radical radiotherapy, Deniaud-Alexandre et al.37 analyzed the effect of adding PET information to CT data through image fusion. Two GTV contours and two corresponding PTVs were drawn by the same physician, the first based on CT data only and the second based on the fused PET-CT images. Nine patients were deemed ineligible for radical radiotherapy based on PET findings of metastatic disease. Of the 92 eligible patients, 21 (23%) had a reduction of GTV after CT-PET fusion with a mean decrease of 42%. A GTV decrease of >25% was observed in seven patients (three with atelectasis). In 24 patients (26%), the GTV was increased, with a mean increase of 26.5%. A GTV increase of >25% was observed in 14 patients. A more recent study published by Faria et al.38 compared the pretreatment chest CT with PET for the radiation therapy treatment planning. A total of 32 patients with proven NSCLC underwent pretreatment chest CT and FDG-PET/CT scans. The authors found that the contour of the GTV of NSCLC patients with coregistered FDG-PET/CT resulted in 18 (56%) of 32 patients with alterations compared with CT targeting.
Because PET-based staging is much more accurate than CT-based staging, and because numerous studies have shown that radiotherapy treatment fields are significantly different if PET is used, we recommend that PET should be used in radiotherapy planning for NSCLC if it is available. Because of the very poor locoregional disease control rates with radiotherapy in lung cancer, there is an increase interest in dose escalation of RT. This could potentially lead to a superior local control and survival, but only if RT is appropriately directed. RTOG 0515 is a radiation treatment planning study for lung cancer patients comparing CT-based GTV contours versus PET/CT based GTV contours. The trial recently completed accrual and the results are not available at this time. The current phase III Intergroup trial (RTOG 0617) evaluating high-dose (74 Gy) versus standard dose (60 Gy) radiation therapy encourages the use of FDG-PET for radiation treatment planning.
HEAD AND NECK CARCINOMA
Traditionally, contrast-enhanced CT and/or MRI scans are the imaging modalities of choice for staging, restaging, and radiotherapy planning for head and neck cancer. They provide morphologic information at high spatial resolution and therefore are used routinely to complement physical examination and endoscopic evaluation of head and neck cancer. FDG-PET also plays a role in the detection of primary tumor, determining lymph node involvement, and assessing the presence of distant metastatic disease.
Perhaps the most important application of FDG-PET in head and neck cancer is for lymph node staging. Metastatic disease to regional (cervical) lymph nodes decreases the overall survival by approximately 50% in patients with head and neck cancer. Detecting nodal metastases at the time of initial presentation affects the choice of treatment and the patient’s prognosis. Radiation treatment planning is directly influenced by the presence of metastatic lymph nodes, both for the radiation dose and for the extension of radiation fields. Therefore, it is crucial to have an imaging modality available that has a high sensitivity in the detection of cervical lymph nodes metastases.
FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY FOR T STAGE ASSESSMENT
MRI has been shown to be more accurate than CT for evaluating the primary tumors of the head and neck, thanks to its high capability to detect soft tissue or bone extension.39 Better visualization of the tumor is translated into smaller interobserver variability in the segmentation of the GTV compared with the results obtained with CT. MRI is now a standard modality to evaluate nasopharyngeal carcinoma,40,41 and it may be superior to CT for assessing oropharyngeal tumors.41 However, the advantage of MRI over CT has not been confirmed for pharyngeal and laryngeal tumors. Both CT and MRI depend on morphologic information for diagnosis and staging. Often the edges of the primary tumor are not well defined due to inflammatory changes around the tumor or due to the low difference in density or signal intensity between the tumor and the adjacent soft tissue. It is possible that in some cases, FGD-PET can provide information that is independent of tumor location and size.
Hannah et al.43 prospectively compared the accuracy of CT and FDG-PET with the histopathologic results in 35 patients with clinically known primary head and neck tumors. Regarding the primary tumor, CT correctly identified 18 of the 35 known primary tumors, with a sensitivity of 51%. False negatives were found in many cases of oral cavity cancer and may be attributable to dental artifacts. FDG-PET, in contrast, had a sensitivity of 88%.
In a larger prospective study, Adams et al.44 reported that FDG-PET identified the primary lesions in 59 of the 60 cases (98% sensitivity). FDG-PET did not detect a primary tumor site in one patient with a small and well-differentiated (T1) squamous cell carcinoma. The authors reported that there was no statistically significant relationship between primary tumor uptake of FDG and tumor grade. Similar results were reported in a smaller study in which PET visualized all of the 22 primary tumors located in the oropharynx and hypopharynx.45 The SUV in the primary tumor was extremely variable, ranging from 2.0 to 13.8 (mean value, 6.3). There was no correlation between tumor size and SUV value, similar to the results of other studies.46 There was no correlation between FDG uptake and histopathologic grading of the primary tumor and lymph node metastases.
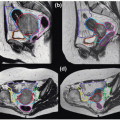
Di Martino et al.47 evaluated the imaging modalities of FDG-PET and CT compared with panendoscopy and histopathologic findings in the diagnosis and staging of 50 patients with head and neck squamous cell primary (n = 37) or recurrent (n = 13) carcinoma. Nine of these patients had an unknown primary tumor. Of the imaging procedures, PET had the highest overall sensitivity and specificity for the detection of both primary tumor and recurrent carcinomas; sensitivity was 95% and 100%, respectively, and specificity was 92% and 100%, respectively. Sensitivity for CT was 68% for primary tumor and 63% for recurrent carcinoma, and specificity was 69% and 80%, respectively. Although sensitivity of panendoscopy for primary tumor and recurrent carcinomas was equal to that of PET, its specificity was 85% for primary tumor and 80% for recurrent carcinoma (Fig. 9.3). PPV for T stage in primary tumor diagnosis was 97% for PET, 86% for CT, and 95% for panendoscopy. In recurrent carcinoma, PPV was 100% for PET, 83% for CT, and 89% for panendoscopy. NPV was 86%, 43%, and 85% for PET, CT, and panendoscopy, respectively, in primary tumor diagnosis, and 100%, 57%, and 100% for PET, CT, and panendoscopy, respectively, in recurrent carcinoma. Therefore, a negative PET scan can exclude recurrent carcinoma with high probability. The false-negative results of CT for diagnosis of recurrent carcinoma were relatively poor, presumably because of alteration in local morphology after irradiation or surgery. Assessing for local recurrence after a procedure that changes morphological tissue characteristics, such as surgery or radiation therapy, may be difficult.
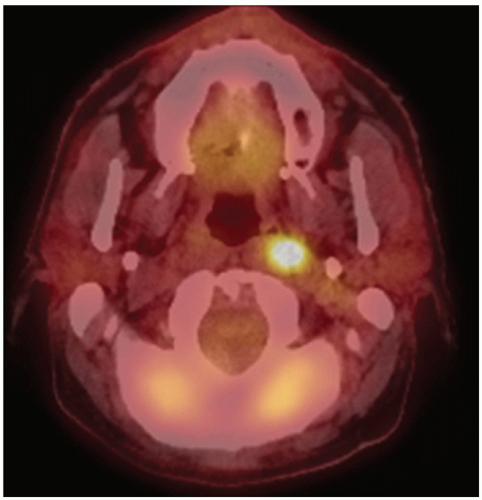
Figure 9.3. This patient underwent panendoscopy with left-sided neck dissection and simple tonsillectomy for “unknown primary” head and neck cancer (tonsillectomy specimen was positive for squamous cell carcinoma [SCC]). Postoperative/preradiation positron emission tomography (PET)/computed tomography (CT) scan showed gross residual disease in the retropharyngeal space, and this received boost irradiation to 70 Gy (with concurrent chemotherapy).
A higher sensitivity for PET compared to CT and MRI in the detection of primary tumor was also reported by Kitagawa et al.48 FDG-PET detected primary tumors in all 23 patients, with a sensitivity of 100%. For MRI and CT, sensitivity was 78% and 68%, respectively. FDG-PET detected small superficial lesions on the tongue, lower lip, and mandibular gingiva in five patients that were not detected by MRI or CT. These results are in agreement with those found in other studies (Fig. 9.4).49, 50, 51
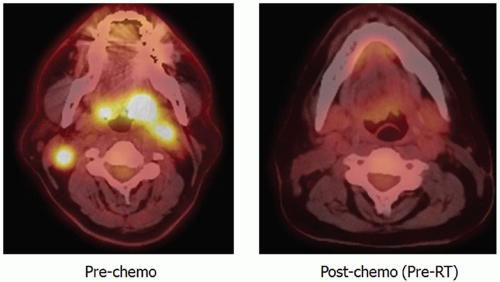
Figure 9.4. This patient with T4N2c base of tongue cancer underwent induction chemotherapy with a complete response. The prechemotherapy positron emission tomography (PET) scan was used for planning subsequent radiotherapy.
FLUORODEOXYGLUCOSE POSITRON EMISSION TOMOGRAPHY FOR N STAGE ASSESSMENT
The detection of metastatic lymphadenopathy in head and neck cancer patients is of critical importance because the presence of nodal metastases is associated with a 50% reduction in 5-year survival. Of note, at least 15% of clinically N0 patients (depending heavily on the primary tumor site) have metastases on pathologic findings. Thus, imaging is important in the pretreatment evaluation of cervical lymph nodes in head and neck cancer patients. Discrimination between reactive enlargement of lymph nodes and metastatic nodes on the basis of morphologic criteria may be problematic. It should be noted that >40% of all lymph node metastases are localized in nodes <10 mm in diameter.52 The calculated sensitivity of CT and MRI for detecting lymph node metastases ranges from 36% to 94%, whereas specificity has ranged from 50% to 98%.53 As described later, FDG-PET may be more accurate than CT or MRI in identifying cervical nodal metastases of head and neck cancer. Table 9.2 lists studies comparing sensitivity and specificity of CT or MRI versus FDG-PET for staging cervical lymph nodes.
TABLE 9.2 Studies Comparing CT/MRI Versus PET for Nodal Staging
Adams et al.44 prospectively evaluated 60 patients to investigate the detection of cervical lymph node metastases of head and neck cancer by FDG-PET and to perform a comparison with CT, MRI, sonographic, and histopathologic findings. Based on histopathologic findings, FDG-PET correctly identified lymph node metastases with a sensitivity of 90% and a specificity of 94%. CT and MRI had a similar performance, visualizing histologically proven lymph node metastases with a sensitivity of 82% and 80%, respectively, and a specificity of 85% and 79%, respectively. Sonography performed with a sensitivity of 72%.
Quantitative analysis of FDG uptake in lymph node metastases using body weight-based SUVs showed no significant correlation between FDG uptake and histologic grading of tumor-involved lymph nodes.
Similar results have been reported in another series.45 The authors prospectively compared the performance of FDG-PET and MRI in 22 patients with oropharynx and hypopharynx squamous cell cancers. The results were compared to pathologic findings in 15 patients. The sensitivity and specificity for detecting individual lymph node involvement were higher for PET than MRI. The sensitivity and specificity were 90% and 96% for PET and 78% and 71% for MRI, respectively. Based on individual lymph nodes, PET correctly identified 75 (90.4%) of 83 histologically proven malignant lymph nodes. Only 19 (4.3%) of 438 benign lymph nodes had increased FDG uptake (presumably as result of inflammatory reactions) and were false positive by PET. MRI had a sensitivity of 78%, correctly identifying 65 (78.3%) of 83 malignant lymph nodes. Because of reactive enlargement, 126 (28.8%) of 438 benign lymph nodes were misinterpreted as malignant, which resulted in a specificity of 71%. To summarize, N stages were correctly identified by MRI in only four patients, whereas PET correctly staged lymph nodes in 15 of 17 patients. PET revealed 16 true-positive and 16 true-negative neck sides with no false-positive and only two false-negative results.
Di Martino et al.47 reported that the overall sensitivity for nodal neck metastases was uniformly 84% both for FDG-PET and CT for initial staging, whereas the sensitivity for staging recurrent nodal metastases was 100% for PET and 67% for CT. Keyes et al.54 reported accurate determination of the presence or absence of metastatic disease in 84% of patients with various primary head and neck cancers in a group of 45 patients.
Hannah et al.43 prospectively compared the accuracy of CT and FDG-PET with the histopathologic reference standard in 35 clinically known primary head and neck tumors. On a level-by-level basis for mapping nodal disease, FDG-PET detected sites of disease accurately in 26 (60.5%) of 43 levels. PET was false positive in five levels in five patients. Spatial inaccuracy of PET contributed to nine false-negative levels and all five false-positive levels and explained inaccuracy in eight patients. On a level-by-level basis, CT detected sites of metastatic disease accurately in 16 (61.5%) of 26 levels. CT was false positive in seven levels in six patients. Intuitively, spatial inaccuracy contributed less to CT inaccuracy than it did to FDG-PET inaccuracy. CT failed to detect any metastatic neck disease in three patients in whom disease was present. In summary, the sensitivity and specificity for the presence of metastatic neck disease on FDG-PET were 82% and 100%, respectively. Sensitivity and specificity for CT were 81% and 81%, respectively.
These data are similar to other smaller studies. Bailet et al.55 reported a sensitivity and specificity for FDG-PET of 71% and 98%, respectively, whereas CT and MRI had a lower sensitivity (58%) and a similar specificity (98%). Braams et al.56 compared PET findings with those of MRI and histologic reference standard. They studied 12 patients with squamous cell cancer of the oral cavity before neck dissection. Sensitivity for PET and MRI was 91% and 36%, respectively; specificity was 88% and 94%, respectively. For the detection of nodal disease, McGuirt et al.57 calculated a sensitivity of 83% and specificity of 82% for PET. Paulus et al.58 retrospectively reviewed 25 patients with biopsy-proven head and neck cancers who underwent CT and FDG-PET examinations prior to treatment. They reported a 50% false-negative rate for FDG-PET. Stokkel et al.49 reported 54 consecutive patients with previously untreated squamous cell carcinoma of the oral cavity and oropharynx. Before surgery, all of the patients underwent CT of the head and neck, ultrasonography with fine-needle aspiration, and FDG-PET. They reported sensitivity for detection of lymph node metastases per neck side of 96%, 85%, and 64% for FDG-PET, CT, and ultrasonography with fine-needle aspiration, respectively. The specificity was 90%, 86%, and 100% for FDG-PET, CT, and ultrasonography with fine-needle aspiration, respectively. Of note, PET detected a second primary tumor in nine patients (17%), which was subsequently confirmed by histologic evaluation.
One hundred six patients with squamous cell carcinoma of the oral cavity underwent FDG-PET, CT, and MRI in a prospective study reported by Stuckensen et al.59 In all patients, tumor was resected and lymph node dissection was performed. The diagnostic procedures showed the following results when compared with the histologic findings: PET had a sensitivity of 70%, specificity of 82%, and accuracy of 75%; CT had a sensitivity of 66%, specificity of 74%, and accuracy of 70%; and MRI had a sensitivity of 64%, specificity of 69%, and accuracy of 66%. These findings suggest that approximately 20% of lymph node metastases are not detectable during pretreatment evaluation. In 10 patients, PET detected either second primary tumors or distant metastases that were not previously appreciated.
Ng et al.60 published a prospective study evaluating the clinical usefulness of FGD-PET, CT, or MRI in 35 patients with oral squamous cell carcinoma with clinically negative neck on palpation. On a level-by-level basis, the sensitivity of FDG-PET for nodal metastases was twofold higher than that of CT/MRI (41% vs. 21.6%). Visual correlation of PET and CT/MRI yielded higher sensitivity (47% vs. 41%) and specificity (98% vs. 96.8%) than FDG-PET alone. The probabilities of occult neck metastases after using FDG-PET were 6.7% in T1 tumors, 10.8% in T2 tumors, 13.3% in T3 tumors, and 25% in T4 tumors; these probabilities decreased to 3.3% in T1 tumors and to 9.2% in T2 tumors after visual correlation with CT/MRI. However, Brouwer et al.61 found a low sensitivity of FDG-PET for the detection of occult lymph node metastases. They studied the diagnostic value of FDG-PET in the detection of occult lymph node metastases, comparing the results of FDG-PET with CT and MRI and the histopathologic outcome of neck dissection specimens from 15 head and neck cancer patients with a clinically negative neck.
Wensing et al.62 suggested that FDG-PET does not contribute to the preoperative workup in patients with oral squamous cell carcinoma and clinically negative neck. In 28 consecutive patients, representing 30 neck dissections, occult metastatic disease was found in 30% of the specimens. Sensitivity, specificity, and accuracy of FDG-PET were 33%, 76%, and 63%, respectively.
Only gold members can continue reading. Log In or Register to continue
May 23, 2016 | Posted by drzezo in GENERAL RADIOLOGY | Comments Off on Positron Emission Tomography/Computed Tomography and Biologically Conformal Radiation Therapy