Site of presentation may depend partially on transplanted organ
Extranodal (80%) > nodal involvement (20%)
• Imaging findings of post-transplant lymphoproliferative disorder parallel those of non-Hodgkin lymphoma (NHL) in immunocompetent patients
• GI tract: Imaging findings are similar to NHL, including mass-like bowel wall thickening, aneurysmal dilatation, ulcerated polyploid mass, or submucosal nodules
Increased prevalence of ulceration and bowel perforation
• Liver: Most frequently involved abdominal solid organ
Single or multiple poorly enhancing masses, discrete mass in porta hepatis, or diffuse infiltration of liver
• Spleen: Splenomegaly ± discrete lesions (usually multiple, hypoattenuating, and variable in size)
• Kidney: Most common site in renal transplant recipients
Heterogeneous mass surrounding hilar vessels, parenchymal masses, or diffuse infiltrative disease
• Nodal disease: Abdominal nodal involvement in only 15-20% of cases
Nodal involvement much less common than in immunocompetent NHL
TOP DIFFERENTIAL DIAGNOSES
• Recurrent or new malignancy
• Opportunistic infections
PATHOLOGY
• Most cases are related to B-lymphocyte proliferation due to Epstein-Barr virus (EBV) infection
CLINICAL ISSUES
• High mortality, with survival rates of only 25-35%
• Treatment: Reduction or cessation of immunosuppression can be effective, although antiviral drugs, chemotherapy, or rituximab may be necessary
(Left) Axial CECT in a patient post liver transplant demonstrates a new hypodense mass in the porta hepatis, as well as an enlarging portacaval lymph node .
(Right) Axial CECT in the same patient demonstrates extensive retroperitoneal lymphadenopathy . The findings of post-transplant lymphoproliferative disorder (PTLD) in this case are indistinguishable from traditional non-Hodgkin lymphoma (NHL) in an immunocompetent patient.
(Left) Axial NECT demonstrates mass-like wall thickening of a segment of colon with aneurysmal dilatation.
(Right) Coronal NECT in the same patient again demonstrates the significant wall thickening of the bowel segment with dilatation. This is a common appearance for both NHL in immunocompetent patients and PTLD.
• Heterogeneous group of lymphoproliferative diseases that occur in post-transplant setting (either solid organ or stem cell transplants), ranging from abnormal lymphoid hyperplasias to frank malignancies
IMAGING
General Features
• Location
Extranodal involvement (80%) is much more common than nodal involvement (20%)
– Unlike lymphoma in general population where nodal disease predominates
Can occur nearly anywhere, with common locations including lungs, GI tract, and CNS
– Site of presentation may depend partially on type of transplanted organ
– Abdominal cavity is most frequently involved (up to 50% of all cases)
– May occur within renal and liver allografts
Some studies have suggested that PTLD may preferentially affect allograft itself
• Size
Masses and nodes range from < 1 cm to huge masses
Imaging Recommendations
• Best imaging tool
CECT for initial diagnosis
PET/CT for staging and follow-up
CT Findings
• Imaging findings of PTLD mostly parallel those of non-Hodgkin lymphoma (NHL) in immunocompetent patients






 in the porta hepatis, as well as an enlarging portacaval lymph node
in the porta hepatis, as well as an enlarging portacaval lymph node  .
.
 . The findings of post-transplant lymphoproliferative disorder (PTLD) in this case are indistinguishable from traditional non-Hodgkin lymphoma (NHL) in an immunocompetent patient.
. The findings of post-transplant lymphoproliferative disorder (PTLD) in this case are indistinguishable from traditional non-Hodgkin lymphoma (NHL) in an immunocompetent patient.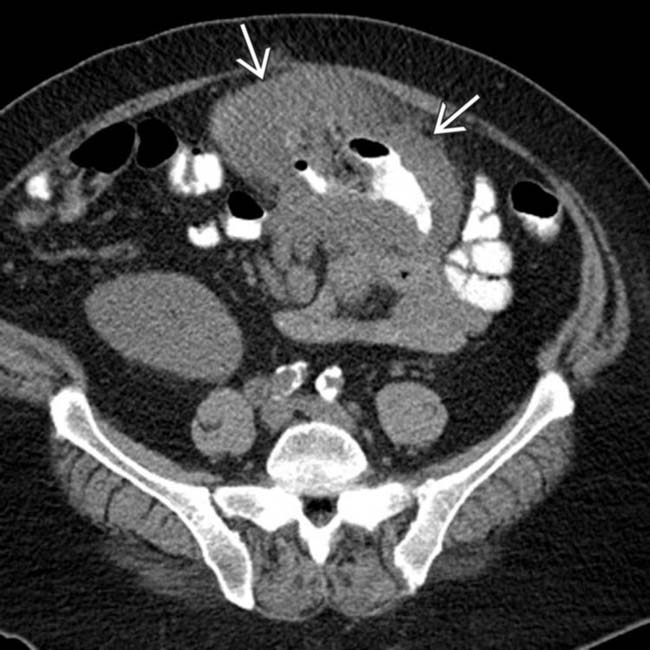
 of a segment of colon with aneurysmal dilatation.
of a segment of colon with aneurysmal dilatation.
 of the bowel segment with dilatation. This is a common appearance for both NHL in immunocompetent patients and PTLD.
of the bowel segment with dilatation. This is a common appearance for both NHL in immunocompetent patients and PTLD.















 Most commonly involved site in renal transplant recipients and may affect native kidneys or allograft
Most commonly involved site in renal transplant recipients and may affect native kidneys or allograft










