Fig. 46.1
Concept and advantage of high-degree posterior rotational osteotomy. The necrotic lesion is moved to the medial to posteromedial non-weight-bearing portion of the joint by high-degree posterior rotational osteotomy. Postoperative uncollapsed anterior viable areas are moved to the loaded portion below the acetabular roof in neutral and flexed positions. After posterior rotation, congruency can be expected in a flexed position of daily life, especially in advanced stages with apparent collapse. The posterior column artery (arrow) is shifted medially and is not under tension without vascular impairment by posterior rotation
46.3 Indications
Indications of posterior rotational osteotomy are as follows: (1) Cases with the necrotic lesion are too far advanced for conservative treatment, or most other joint-preserving operations are not effective. (2) Cases with less than one-third of the viable posterior portion of the femoral head which are out of indication for conventional anterior rotational osteotomy. (3) In young patients with extensive collapsed lesion where less than one-third of anterior and posterior portion remain viable area, “high-degree” posterior rotational osteotomy might be required even if joint space narrowing already occurred [10–14].
46.3.1 Preoperative Assessment
The posterior rotational angle and intentional varus angle necessary for this procedure were determined by preoperative assessment, mainly on radiographic findings and magnetic resonance imaging (Fig. 46.2). Lateral radiographs should be taken in all hips by the method described by Sugioka [9] to observe the location and extent of necrotic region. The patients are laid in supine position; radiographs of hips were taken in 90° of flexion, 45° of abduction, and neutral rotation. This radiograph was available for decision of indications in 90° anterior or posterior rotational osteotomy. In addition, anterior-posterior radiographs in a flexed position were obtained. The patients are laid in supine position, and the affected hip was flexed with 45° of abduction with varying degrees of flexion [13, 14] (Fig. 46.3a). Location of the necrotic lesion was carefully confirmed on radiographs in various flexion positions. At that time, flexion angle could reveal the posterior rotational angle. By the use of this radiograph, the varus angle was decided by drawing a figure.
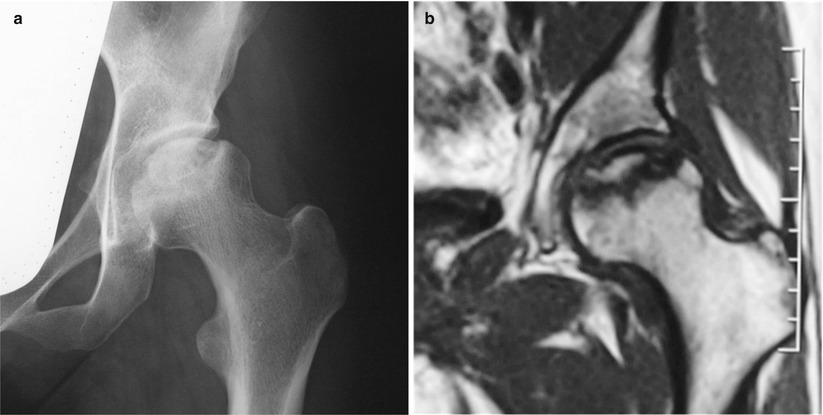
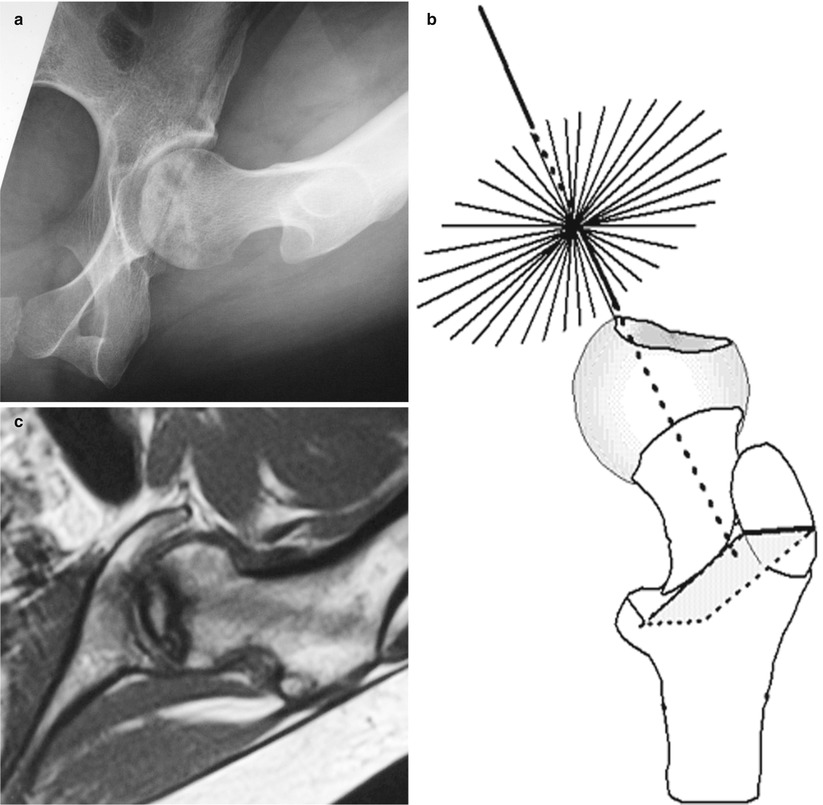
Fig. 46.2
A 27-year-old woman having high dose of corticosteroids due to treatment of sclerotic lupus erythematosus. (a) Preoperative anteroposterior radiograph of her left hip showed large collapsed extensive lesion. (b) Magnetic resonance imaging (T1-weighted image) coronal slice showed extensive low-intensity area below acetabular roof
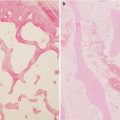
Fig. 46.3
Radial MRI and AP radiographs in a flexed position in the patient of Fig. 46.2. (a) AP radiograph in 120° flexion with 45° of abduction showed anterior viable area that is moved to loaded portion. (b) Radial MRI was developed for decision of location of viable, necrotic area, and rotational angle was taken perpendicular to the axis of the femoral neck 10° each. (c) Radial MRI equivalent of 120° posterior rotation indicated the anteroinferior viable portion implied by normal intensity
Magnetic resonance imaging can be available if the demarcation area between living and necrotic bone is not clearly visualized on radiographs. Radial MRI (Fig. 46.3b, c) was developed for decision of location of viable necrotic area, and rotational angle, T1-weighted image, and T2 fat suppression image were taken perpendicular to the axis of the femoral neck 10° each (Fig. 46.3b). MRI findings were compared with radiographic findings; then, posterior rotational angle and intentional varus angle were decided.
46.4 Operative Technique
A modified Southern approach [10–14] was used with the patients in the lateral position. Skin incision was performed from distal to the anterior superior iliac spine and extended distally and posteriorly, passing through the distal portion of the greater trochanter. The fascia is incised in line with the skin incision. With the hip rotated internally, the short external rotators are incised at the acetabular margin. The location of the posterior column vessels should be carefully confirmed. The obturator externus is elevated and incised, protecting nutrient vessels. The posterior column vessels are situated along the obturator externus. The greater trochanter is osteomized and is reflected proximally with the gluteus medius and minimus. The complete incision of the iliopsoas tendon is necessary in area attached to the lesser trochanter. The capsule was exposed widely; then, the capsule is incised circumferentially except the anteroinferior portion.
Method of Decision for Osteotomy Plane: The hip is rotated internally; position with maximum lengths of femoral neck is confirmed under image intensifier, and then, one K-wire is placed into the center of the femoral neck through the trochanteric osteotomy [13]. Two additional K-wires are inserted into the intertrochanteric area, perpendicular to the axis of the femoral neck to decide the correct osteotomy plane. This technique is different from original technique described by Sugioka [9] (Fig. 46.4). A Steinman pin is inserted into anterior portion of the femoral neck. The femoral head and neck is rotated manually to posterior direction. Then, the remained anteroinferior capsular ligament (mainly the iliofemoral ligament) is detached from the femoral neck [13].
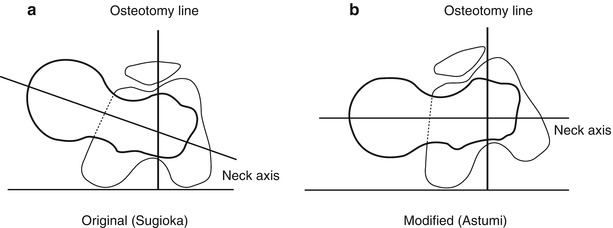
Fig. 46.4
Method of decision for osteotomy plane. The hip is rotated internally; position with maximum lengths of the femoral neck is confirmed under image intensifier; then, one K-wire is placed into the center of the femoral neck through the trochanteric osteotomy. Two additional K-wires are inserted into the intertrochanteric area, perpendicular to the axis of the femoral neck to decide the correct osteotomy plane (b). This technique is different form original technique described by Sugioka. The osteotomy plane described by Sugioka (a) is oblique to the femoral neck axis
The image intensifier is used for the final determination of the correct position [10, 12, 13]. Bleeding from the osteomized area of proximal portion should be confirmed. Fixation of the transtrochanteric osteotomy is performed by screws and plate system designed by Atsumi [10, 12, 13]. For postoperative management, early motion exercises and isometric exercises of the quadriceps muscle were performed immediately after the patients became free from postoperative pain. The patients were in bed for one week and then used a wheel chair. Partial weight bearing was initiated 5–6 weeks after operation using 2 crutches. Walking with 1 crutch should be continued 6 months after operation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


