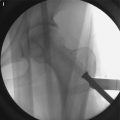
Fig. 15.1
Plain radiographs of a 45-year-old man with right femoral osteonecrosis show linear sclerosis (arrow) in the right femoral neck (a, b). These look like a femoral neck fracture pattern (High signal intensity bandlike lesion, indicated by arrow) on MRI image (c), but bone scan images show the characteristics of avascular necrosis with photon defect and increased uptake of subcapital area (d)
Fig. 15.2
Serial radiographs of anterior rotational trochanteric osteotomy from a 16-year-old man with posttraumatic osteonecrosis of the femoral head are shown
Fig. 15.3
Gluteus medius muscle pedicl bone graft from iliac crest (a, b) and from greater trochanter (c, d)
Fig. 15.4
Serial pinhole bone scintigraphy after vessel-pedicle bone graft for osteonecrosis of the femoral head shows gradually increasing uptake in the femoral head
Fig. 15.5
Three cases of posttraumatic osteonecrosis development are shown
Treatment in both posttraumatic and nontraumatic osteonecrosis is very similar. The choice of treatment will depend on patient age, gender, extent of necrosis, and location of osteonecrosis.
15.2 Incidence of Posttraumatic Osteonecrosis
Hip trauma is a major risk factor of osteonecrosis together with steroid, alcohol, and connective tissue diseases. The risk increases with the degree of displacement and comminution of fracture and dislocation. The risk of osteonecrosis also increases as the fracture line moves closer to the head, and subcapital fractures have the maximum risk of osteonecrosis [5–10].
The incidence of osteonecrosis after dislocation, which is reported to be in the range of 10–25 %, varies depending on the severity of injury of the associated femoral head or acetabular fractures [11]. Eighty-five to ninety percent of hip dislocations are posterior dislocations with or without other associated femoral head injuries [12]. Hougaahou et al. [4] reported that the incidence of osteonecrosis was 4.8 % when anatomical reduction was performed within 6 h after dislocation, while the percentage rose to 52.9 % when the reduction was performed after 6 h.
The incidence of osteonecrosis after a displaced femoral neck fracture is reported to be 15–20 % [13–16]. The discrepancies in the reported incidence reflect variation with fracture types, accuracy of reduction, and time to reduction.
Osteonecrosis can occur in neck fractures whether the fracture occurs at the intra- and extracapsular level. In general intracapsular fractures are at higher risk compared to extracapsular fractures [17, 18]. The actual incidence may be estimated to be higher considering the possibility of follow-up loss or overlooked reports of osteonecrosis after pertrochanteric fractures in the literature [19].
15.2.1 Factors Related to the Incidence of Osteonecrosis
15.2.1.1 Age
Age is a suspected, but unconfirmed, factor related with the incidence of osteonecrosis [13, 20–23]. Some researchers claimed that the incidence of posttraumatic osteonecrosis is positively correlated with age [20, 21], while another study reported that the incidence decreased after 75 years of age [13]. This may reflect the fact that in younger people these injuries often occur after high-energy trauma, with associated damage to soft tissue and vascularity similar to nontraumatic osteonecrosis, in contrast to more elderly individuals in which injuries typically occur after low-energy trauma. These research findings suggest that the estimated incidence of osteonecrosis is high after intracapsular fractures that occur among adults under 50 years of age. It is very important to determine the best treatment, especially in young patients who have a long life expectancy and high activity level.
15.2.1.2 Degree of Displacement and Reduction
The degree of displacement in the intracapsular fracture is closely related with the development of osteonecrosis. In Garden’s classification, without displacement is classified as Type 1 and 2 and with displacement is classified as Type 3 and 4. This classification helps to predict development of osteonecrosis [14]. Researchers have reported a strong correlation between the development of avascular necrosis and fragment displacement [24]. This suggests that damage in reticular arteries caused by displacement of bone fragments or posterior dislocation plays an important role in the development of posttraumatic osteonecrosis.
The degree of reduction in femur neck fracture is determined based on the Garden’s alignment index, which refers to the angles of the medial cortex line and proximal trabeculae bundle axis on a radiograph of the anterior and posterior segments of hip joints. An acceptable range of 150–185° insures maximum chances of union and minimum chances of osteonecrosis [8, 25, 26]. However, severe comminuted fracture of the femoral neck or malrotation and/or unstable fixation may negatively affect revascularization of the head and may lead to osteonecrosis [14]. Sustained traction or excessive internal/external rotation of the hip, especially if maintained for a long time before surgery, may damage the lateral femoral circumflex artery causing osteonecrosis [27–30].
To decrease risk of damage of the major vessels, it is preferable to avoid excessive extension or internal rotation of the hip joint [28–32]. Several reports recommended that the removal of intracapsular hematoma improves blood flow of the femoral head and decreases the development of osteonecrosis [33–35].
Every reduction after traumatic hip dislocation is also important to prevent osteonecrosis. Sanders et al. [9] found that the incidence of osteonecrosis was 4.8 % when reduced within 6 h and 52.9 % when reduced after 6 h. Similarly, Yeranosian et al. [36] also reported that when the reduction was achieved within 24 h, osteonecrosis progression was four times less as compared to patients in whom reduction was achieved after more than 24 h. These findings emphasize the significance of early reduction in hip joint dislocations.
15.2.1.3 Timing of Surgical Intervention
It is still controversial whether delay of surgery increases the incidence of osteonecrosis when treating neck fractures [37, 38]. There is a close correlation between delayed treatment and onset of traumatic osteonecrosis of the hip [39, 40]. It was recommended that traction for the neck fracture should be kept in flexion position to decrease intracapsular pressure before surgery [30]. In contrast, another report claimed that early preoperative reduction of the fracture using splinting or traction of a limb did not affect outcome and no correlation was found between the development of osteonecrosis and the time to surgical intervention after trauma. The authors recommended a good preoperative plan and achievement of a stable and anatomical reduction during operation because these aspects are more important than early surgery [38]. More evidence needs to be collected more a definitive conclusion is reached.
15.2.1.4 Type of Surgery
The type of surgery also affects the development of osteonecrosis. The incidence of posttraumatic osteonecrosis reportedly decreased significantly when less invasive procedure and the accurate reduction was achieved [29]. Garden et al. reported that the results of follow-up of 500 cases of subcapital femoral neck fracture showed a decrease in the incidence of osteonecrosis depending on the skills and experience of the surgeons [14]. The fixation methods affected the incidence of osteonecrosis based on a study of 219 patients with femoral neck fracture in which four different fixation methods were used [37].
The majority of displaced neck fractures require open reduction and internal fixation. However, during the intraoperative femoral head screw fixation, the remaining retinacular vessel can be damaged if the head rotation is not precise. The lateral circumflex artery can be damaged during intramedullary nail insertion in pertrochanteric or subtrochanteric fracture [41]. Thus, at the time of a internal fixation, the surgeon should be careful about malrotation of the femoral head. Attention should be paid to avoid retinacular artery damage when intramedullary nailing is performed.
In older patients with a femoral neck fracture, arthroplasty as a primary treatment has been performed to avoid secondary surgery because of later osteonecrosis or nonunion. Patient’s age is one of the crucial factors for the choice of treatment in femoral neck fracture. Primary arthroplasty rather than internal fixation is preferred in older patients with femoral neck fracture [42]. Bipolar hemiarthroplasty has advantages of shorter surgery time and lesser bleeding compared with total hip arthroplasty. However, since some patients complain of groin pain after bipolar hemiarthroplasty, total hip arthroplasty is increasing [43].
15.3 Diagnosis of Posttraumatic Osteonecrosis
15.3.1 Signs and Symptoms
Most patients with osteonecrosis may not present clinically until later stages. Some patients may remain asymptomatic even in the stage of segmental collapse. The pain in osteonecrosis is usually located in the inguinal/gluteal/proximal femoral region. However, it is commonly neglected by patients and wrongly attributed to previous trauma. Therefore it is important that clinician differentiate these symptoms very carefully. Long-term follow-up of these patients is important as segmental collapse can occur as late as 2 years after injury [8, 13]. It is impossible to detect early osteonecrosis in patients with nontraumatic osteonecrosis, while early diagnosis is possible by interval checkup in patients with posttraumatic osteonecrosis. Therefore, compared with patients with nontraumatic osteonecrosis, proper treatment can be provided to patients with posttraumatic osteonecrosis.
15.3.2 Imaging
15.3.2.1 X-ray
X-ray diagnosis of posttraumatic osteonecrosis is very similar to nontraumatic osteonecrosis. When a diagnosis of early stage of osteonecrosis is considered using X-ray, the reported sensitivity of radiologic diagnosis in the early stage is around 41 % [44]. It takes 1–5 years for the pathology of osteonecrosis to progress and produce abnormalities that are apparent on X-ray, and posttraumatic osteonecrosis usually does not appear until 1–2 years after injury. Some reports suggested that most patients show radiologic changes of osteonecrosis within 2–3 years after trauma, while others reported the osteonecrosis was detected at 11–24 months after the internal fixation on plain radiography [7, 13, 14, 16, 45]. Considering these dichotomous reports, osteonecrosis should not be ruled out after a simple check of X-ray with normal appearance, and all patients should be followed up for a protracted time.
If osteoclastic resorption overlaps with new bone formation on the revascularized area, it is evident as mottled density on the X-ray. If the femoral head is collapsed, increased density is evident in the compacted area. Subchondral sclerosis or lucency also suggests osteonecrosis. This may be caused by increased density or osteoporosis in bone tissue where blood is not supplied. In cases of associated nonunion, radiologic changes and late femoral head collapse may be further delayed due to the absence of the revascularization process.
The best view for the femoral neck can be obtained by anteroposterior radiographic view with 15° internal rotation of the hip joint in the supine position. For a clearer view of the femoral head, it is necessary to check the femoral head lateral view, because femoral head collapse and crescent sign (subchondral facture sign) in early stages are mainly detected in the anterosuperior segment of the femoral head. The patient is laid in the supine position with the hip in 90° flexion and 45° abduction. The X-ray beam is directed from anterior to posterior. If the metallic implant blocks the necrotic lesion of interest on the X-ray, the patient’s position may be changed to obtain a better view. The radiographic images are only a basic standard for examination. Magnetic resonance imaging (MRI) and bone scan should be added for precise and definite diagnosis.
15.3.2.2 MRI
MRI is considered to be the most effective diagnostic tool for the diagnosis of nontraumatic osteonecrosis and traumatic osteonecrosis because of its specificity and sensitivity [46, 47]. MRI can detect bone marrow change very early and can predict its progression. MRI has a higher sensitivity than computed tomography (CT) or radionuclide bone scintigraphy [48, 49]. Glickstein et al. [46] reported MRI specificity and sensitivity of 98 and 97 %, respectively. Diagnoses can be made on the T1-weighted axial localizer and T1-weighted or T2-weighted spin-echo coronal images. The necrotic margin is evident as a single line on T1-weighted images and a double line on T2-weighted images. The double-line sign is a specific and pathognomonic sign also in nontraumatic osteonecrosis, and it is seen in concentric low- and high-signal-intensity bands on the T2-weighted image [50].
MRI has a 96.7 % accuracy compared with the pathologic diagnosis of core biopsy [47]. Even though MRI patterns do not exactly match radiographic stages, MRI can provide all the information necessary for diagnosis and clinical staging, while the bone scan offers limited information [51, 52].
Contrary to general beliefs, internal metallic fixation does not cause any problems in MRI imaging because most metallic implants do not have a ferromagnetic property. However, metallic implants have different susceptibility between metallic implants and surrounding tissues which could cause a geometric distortion known as the susceptibility artifact. If an internal metallic fixation is in place after the injury, it leads to image distortion making diagnosis difficult [48, 53]. The cause of the problem is the nonlinearity that characterizes metal elements. Nonlinearity resulting from pixel shift and intensity variation can lead to serious distortions in images [46, 49, 51, 52, 54–57].
This susceptibility artifact is determined by the composition of metallic devices and the different MRI parameters such as the orientation of devices in relation to direction of the main magnetic field, type of pulse sequence, voxel size as determined by the field of view, image matrix, section thickness, and echo train length [47, 50, 57–60]. Titanium implants create fewer artifacts than stainless steel implants [47]. Bagheri et al. [61] reported fewer artifacts with increasing duration after surgery with metallic implants. Artifacts remain a significant problem in MRI. Some artifacts remain, even when the implants are removed [62].
There are few reports about the MRI findings in posttraumatic osteonecrosis. Speer et al. [63] reported that a two-dimensional Fourier transform spin-echo technique detected no changes in the first 48 h after intracapsular neck fracture. Along the same line, another study reported that no significant changes or histological necrosis were detected even after the first 65 days. Kamano et al. [64] reported on the three patterns on the T1 and T2 fat saturation images taken 24.5 h after femur transcervical neck fractures. Type I, which revealed non-enhancement, was related to necrosis in all cases, while type III showing a total enhancement was linked to femoral head viability in all patients. Type II which reveals partial enhancement was related with osteonecrosis in five of 12 cases. In the report of Sugano et al., MRI was done 1, 6, and 12 months after internal fixation in 17 cases of femur neck transcervical fracture [65]. At 1 month after the surgery, a low signal was detected in T1 and high signal in T2 in eight cases. The authors identified three different types of images: small upper lateral infarction was classified as type 1, narrow upper lateral lesion extending to the fovea as type 2, and wide lesion taking up most of femoral head as type 3. All 17 cases were observed to have abnormalities on MRI. None of the cases in type 1, 75 % cases in type 2, and all the cases in type 3 progressed to necrosis. In the report of Kawasaki et al. on femur neck transcervical fracture, T1-weighted MRI and plain radiographic images were taken at 1, 2, 6, and 12 months after internal fixation [45]. On the images taken 2 months after the procedure, eight of 31 cases showed band-like images; on the images taken in 6 months, 12 cases showed band-like images. Among the band-like images classified as B1 (lateral), B2 (superficial), B3 (intermediate), and B4 (extensive), necrosis was related to the B2, B3, and B4 bands. It was also related to Garden types 3 and 4. Specificity and diagnosis accuracy was 100 and 87 %, respectively.
15.3.2.3 Bone Scan
Planar scintigraphic imaging has a sensitivity ranging from 47.8 to 78.3 %. Despite the fact that sensitivity is low at stages I and II, planar scintigraphic imaging has several strengths. It has no false-positive imaging and is useful in patients with cardiac pacemakers or intracranial clips or who suffer from claustrophobia, for whom MRI is not indicated [66]. Bone scintigraphy can detect early osteonecrosis even when MRI does not detect the necrotic changes [67, 68]. Maillefert et al. [66] reported that bone scintigraphy with a pinhole collimator has a better sensitivity in diagnosing osteonecrosis compared with bone scintigraphy. Turner et al. [69] reported that technetium-99m antimony colloid as a radionuclide does not stop additional osteogenesis by binding with subendothelial dendritic macrophages. According to the authors, uptake of technetium-99 m antimony colloid decreases after bone fracture and devascularization. The uptake increases as the necrosis progresses, and vascularity and bone activity increases. According to Dong et al. [70], nuclide uptake increases 3–4 months after surgery and peaks 6–12 months after surgery.
A pinhole collimator is a type of a conical collimator having a small circular aperture (3–5 mm). A pinhole collimator produces an inverted image as a photographic camera does. This image can be enlarged so that even a small structure can be detected, contributing to diagnosis of scintigraphic abnormality. A pinhole collimator increases the resolution of circumscribed areas, and its acquisition time is just 15 min, while SPECT scanning takes 45 min. Planar scintigraphic imaging using quantitative bone scanning offers physiologic data not possible in MRI and also makes uptake quantification available at perfusion and static phase. Therefore, when the patients with head-preserving surgery were followed for revascularization, planar scintigraphic imaging is most useful than any other diagnostic tools [66].
15.4 Treatment
15.4.1 General Considerations for Choosing Treatment
As in the treatment of nontraumatic osteonecrosis, the ultimate goal of treatment for posttraumatic osteonecrosis is to preserve the femoral head, especially in young patients. However, arthroplasty has been widely used with great development of surgical procedures, implants and their materials, high survival rates and patient satisfaction. Clear differentiation of indications between arthroplasty and head salvage procedure is still controversial, and a grey zone still persists. Even though arthroplasty shows good prognosis in most cases, there are some related complications that include joint infection, osteolysis, and aseptic loosening. These compromise the longevity of total hip arthroplasty.
Femoral head-preserving surgery should be considered for young patients, especially adolescent patients, when a surgeon decides on treatment of posttraumatic osteonecrosis considering the remaining life expectancy and high activity of patients.
Osteotomy has been one of the methods preserving the femoral head in osteonecrosis. If the necrotic lesion is anteriorly or posteriorly shifted, rotational trochanteric osteotomy may be one choice. If the lesion is medially or laterally shifted, varus osteotomy or valgus osteotomy can be performed.
After the head-preserving surgery, the healing period until ambulation is around 3 months. On the other hand, total hip arthroplasty is usually shorter in the healing period than that of head-preserving surgery. For this reason, there are some patients who prefer total hip arthroplasty because the patients have to return to work soon. If a patient who has suffered osteonecrosis desires an early return to daily life, even if head-preserving surgery is more appropriate for the patient, total hip arthroplasty may be indicated.
Total hip arthroplasty may be considered inevitable in cases with large necrosis or serious collapse. Regarding the bearing surface for total hip arthroplasty, ceramic-on-ceramic surface is recommended to reduce complications such as aseptic loosening or osteolysis, especially in young patients [71].
In determining the surgery for the osteonecrosis, the age of the patient; severity, extent, and location of necrosis; and socioeconomic needs of the patient should be considered carefully. Surgeon’s ability to perform head-preserving surgery seems one of the factors to be considered in the decision process.
15.4.2 Head-Preserving Procedures
Electric shock wave shows some effects on the treatment of osteonecrosis but no established conclusion is possible yet. Wang et al. showed that in patients with the ARCO I, II, and III osteonecrosis, treatment with extracorporeal shock wave had better results than treatment with core decompression and nonvascularized fibular grafting. They postulated that shock wave induces hyperstimulation analgesia by increasing threshold of pain and promotes bone healing as a result of microfracture [72]. Further prospective studies with reliable clinical data are required for wide clinical application.
15.4.2.1 Bisphosphonate
Bisphosphonate can be effective for patients with posttraumatic osteonecrosis if it is used together with other means of treatment [72–76].
The use of bisphosphonate for nontraumatic osteonecrosis both enhances the apoptosis of osteoclasts and reduces the apoptosis of osteoblasts, thus blocking the progression of bone resorption and collapse. Similar effects have been observed among posttraumatic osteonecrosis patients. Agarwala et al. [73] reported that the use of bisphosphonate brought about functional improvement and helped prevent osteonecrosis progression in their study based on 69 cases of hip osteonecrosis including five cases of posttraumatic osteonecrosis. However, the study reported that the result was unsatisfactory for the osteonecrosis where collapse was already in progress. Ramachandran et al. [74] also found in their clinical study of 28 posttraumatic hip cases that bisphosphonate led to a delay in osteonecrosis progression.
In recent years, cocktail therapies that use bisphosphonate together with extracorporeal shock wave therapy, electrical shock wave therapy, hyperoxygen therapy, and nonsteroidal anti-inflammatory drug have been suggested for femoral head necrosis of the hip [72, 75]. Bisphosphonate has been avidly investigated. In treatment of osteonecrosis of the hip, comparison of extracorporeal shock wave with shock wave and alendronate and the proper volume of bisphosphonate and period for using are not established yet [76]. But, research on bisphosphonate suggests that its use for the treatment of patients in a relatively early stage of posttraumatic osteonecrosis could be justified.
15.4.2.2 Viable Bone Grafting
Viable bone grafting that has been used for nontraumatic osteonecrosis can also be a good method treating traumatic osteonecrosis. Many reports introduced several bone graft methods including autograft or central decompression combined with allogeneic transplantation. Free vascularized fibular grafting for the treatment of osteonecrosis of the femoral head was first described in the 1970s [77]. Later Phemister [78] reported success rate of 70 % using vascularized fibular graft; Zhang et al. [79] reported that free vascularized fibular grafting was worthwhile for teenagers with posttraumatic osteonecrosis, even though collapse of the femoral head had reported that through this method, pain relief and restoration of the sphericity of the femoral head could be expected. Even though the vascularized fibular grafting had good results in atraumatic osteonecrosis in early stages, recently these methods are not used widely due to the unpredictable results and complicated surgical technique.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


