(1)
Department of Radiology, John H Stroger Jr Hospital of Cook County, Chicago, IL, USA
Thrombotic Embolism
Diagnosis
Acute Pulmonary Embolus
Imaging Features
1.
Intraluminal filling defect
2.
Occluded artery larger than the adjacent patent arteries
3.
Doughnut sign in short axis, tram track sign in long axis of artery, thrombus surrounded by contrast-filled blood
4.
Eccentric filling defect forming acute angle with wall
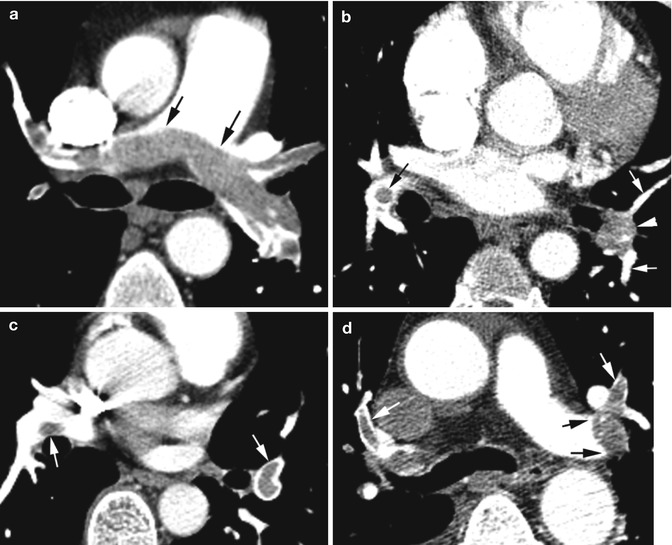
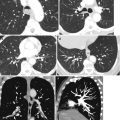
Fig. 1.1
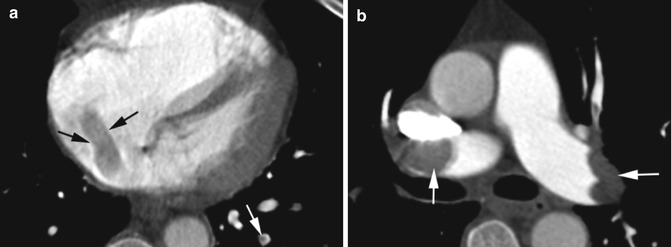
Acute pulmonary embolus. CECT axial images show (a) saddle thrombus (thin black arrows) involving the right and left main pulmonary arteries across the bifurcation. (b) Enlarged left lower lobe pulmonary artery (arrowhead) filled with thrombus and larger than adjacent patent arteries (white arrows). Doughnut sign in the right lower lobe pulmonary artery (black arrow). (c) Doughnut sign in the right and left lower lobe pulmonary arteries (arrows). (d) Eccentric thrombus causing filling defect with acute angle with wall in the left lower lobe pulmonary artery (black arrows). Tram track sign in both upper lobe pulmonary arteries (white arrows)
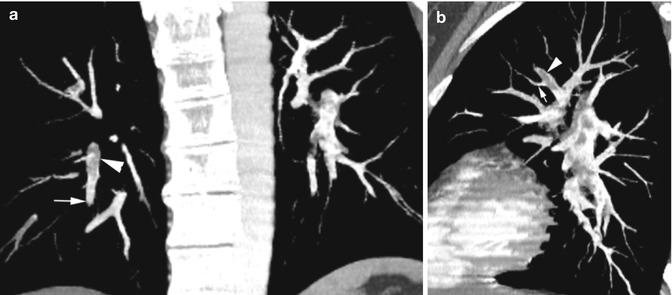
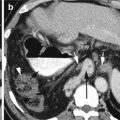
Fig. 1.2
Acute pulmonary embolus. (a) Coronal and (b) sagittal reformatted CT shows portion of artery with thrombus larger (arrowhead) than the distal portion and the adjacent arteries (thin white arrow)
Ancillary findings of acute pulmonary embolus
1.
Hampton’s hump—pleural-based, wedge-shaped areas of consolidation may represent infarction
2.
Linear atelectasis, regional oligemia, pleural effusion
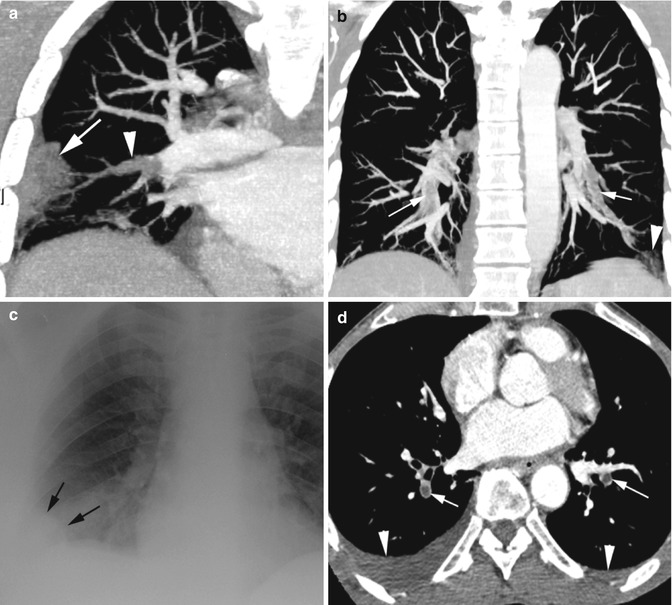
Fig. 1.3
Hampton’s Hump. (a) Axial CT shows thrombus in the right lower lobe pulmonary artery (arrowhead) with peripheral wedge-shaped pleural-based increased density due to infarction (arrow) forming Hampton’s hump. (b) Coronal reformatted image shows thrombus in multiple lower lobe arteries bilaterally (arrows) with wedge-shaped infarction in left costophrenic angle (arrowhead), the Hampton’s hump. (c) Chest X-ray of Hampton hump in a different patient with history of PE shows a convex blunting of right costophrenic angle (black arrows). (d) Axial CT in different patient shows embolus in the lower lobe pulmonary artery bilaterally (arrow) with pleural effusion (arrowheads) bilaterally more on the right side
Assessment of severity and prognosis of PE—right heart strain

1.
Short axis ratio of RV/LV in diastole at the level of valves >1 and >1.5 indicates severe episode.
2.
Leftward bowing of interventricular septum.
3.
Reflux of contrast into IVC.
4.
Diameter of MPA more than 29 mm.
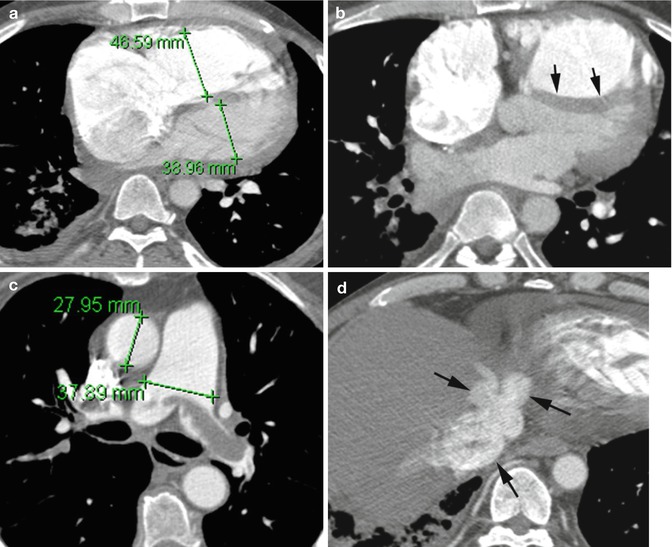
Fig. 1.4
Right heart strain. Axial CT (a) short axis ratio of the right ventricle and left ventricle at the level of the valves is more than one. (b) Leftward deviation of the interventricular septum (arrows). (c) Pulmonary artery-to-aorta ratio greater than one and with saddle thrombus. (d) Reflux of contrast into IVC and hepatic veins (arrows)
Fig. 1.5
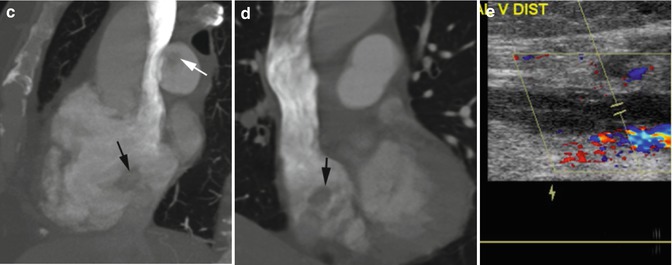
Acute PE with thrombus in RA and popliteal vein. (a) Axial CT shows thrombus in RA as well marginated filling defect (black arrows). Thrombus is also seen in the lower lobe pulmonary artery (white arrow). (b) Axial CT shows thrombus in both main pulmonary arteries (arrows). (c, d) Sagittal and coronal reformatted images show thrombus in the RA (black arrow) and right main pulmonary artery (white arrow). (e) Doppler US shows echogenic thrombus distending the left popliteal vein (cursor) with lack of color and spectral flow
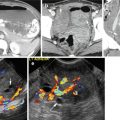
Fig. 1.6
Hepatocellular carcinoma (HCC) invading the left portal vein with PE in the right lower lobe. Axial CT: (a) Arterial phase shows enhancing tumor thrombus in the left portal vein (black arrow). Multicentric HCC is seen in the rest of the liver (white arrows). (b) Portal venous phase shows high-density thrombus in the portal vein (arrow). (c) Coronal reformatted image shows tumor vessels in the tumor extending into the portal vein (arrows). (d) Axial CT shows pulmonary emboli in the right lower lobe pulmonary arteries (arrows)
Diagnosis
Chronic PE
A.
Vascular CTPA signs
1.
Pulmonary artery findings:
(i)
Complete obstruction
(ii)
Get Clinical Tree app for offline access

Partial filling defects:
(a)
Organized thrombus runs parallel to arterial lumen, causing thickened wall and irregularity of intima
(b)
Obtuse angle with vessel wall in transverse plane
(c)
Poststenotic dilatation or aneurysm can occur
(d)




Abrupt vessel narrowing by recanalization or stenosis by organized thrombus
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree