PULMONARY EDEMA
Fluid accumulation in the lungs may be the result of changes in pulmonary venous hydrostatic pressure, increased permeability of capillary endothelium, or a combination of these two. The HRCT features of these two processes show significant overlap and are often difficult to distinguish. The most important role of HRCT is in making a distinction between edema and other causes of pulmonary symptoms, such as pneumonia.
Hydrostatic Pulmonary Edema
An alteration of the hydrostatic or oncotic pressure within pulmonary capillaries may result in pulmonary edema. Increased hydrostatic pressure is significantly more common and usually results from pulmonary venous hypertension due to left heart disease. Left heart failure and valvular heart disease are the most frequent causes. Decreased oncotic pressure due to low albumin may also result in edema accumulation, but this is less common.
The HRCT findings of hydrostatic pulmonary edema associated with pulmonary venous hypertension are shown in Table 8.1. Hydrostatic pulmonary edema may be interstitial or alveolar. These may both be associated with vascular congestion in which the pulmonary veins are enlarged, particularly in the upper lobes, and both are typically diffuse or symmetrical.
Interstitial Pulmonary Edema
Edema fluid may accumulate within the interlobular septa, subpleural interstitium, and peribronchovascular interstitium.
On HRCT, edema fluid within the interlobular septa appears as smooth interlobular septal thickening (Fig. 8.1). Keep in mind that a few interlobular septa may be seen in normal patients. However, when multiple, easily seen, interlobular septa are visible, the septa are abnormally thickened. Interlobular septal thickening can be diagnosed if visible reticular opacities outline what can be recognized as pulmonary lobules because of their typical size and polygonal shape. Centrilobular arteries may be seen as small dots at the center of these polygonal structures. Interlobular septal thickening as a result of edema is often best seen in the upper lobes, because septa are best developed in this location. Subpleural edema (Fig. 8.2), equivalent to interlobular septal thickening, may be seen as thickening of fissures.
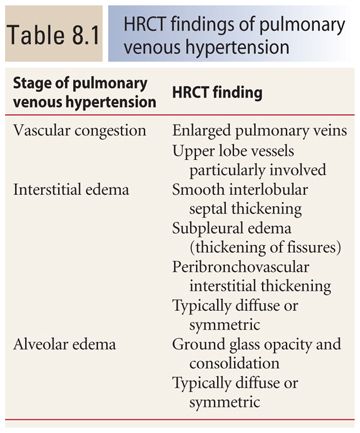

Figure 8.1
Pulmonary edema with smooth interlobular septal and fissural thickening. Multiple, smooth, thin, interconnecting linear opacities are noted, outlining polygonal structures, which can be identified as pulmonary lobules because of their characteristic size and shape and the presence of a centrilobular artery. These are the interlobular septa that marginate the pulmonary lobule. Pulmonary edema is the most common cause of this finding. Thickening of the major fissures is also seen.
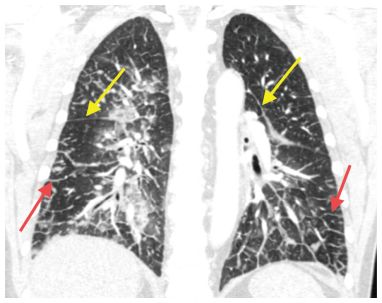
Figure 8.2
Pulmonary edema with interlobular septal and fissural thickening. Coronal reformatted CT shows thickening of the fissures (yellow arrows). This represents fluid in the subpleural interstitium. Smooth interlobular septal thickening is also noted (red arrows) in this patient with interstitial pulmonary edema.
Edema fluid may also accumulate in the peribronchovascular interstitium. This may be the result of lymphatic drainage of edema fluid to the hila. On HRCT, thickening of the interstitium surrounding the central bronchi gives the appearance of bronchial wall thickening and a corresponding increase in the diameter of pulmonary arteries (Fig. 8.3).
Smooth interlobular septal and peribronchovascular interstitial thickening are often seen in association with findings of alveolar edema (Fig. 8.4). Their distribution is quite variable, but findings tend to be bilateral and relatively symmetric. While edema is often most severe in the dependent lung regions, this is not a constant feature.
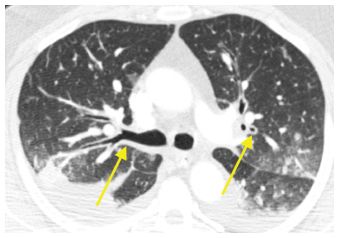
Figure 8.3
Pulmonary edema with peribronchovascular interstitial thickening. Fluid is seen in the interstitium adjacent to or surrounding the bronchi and arteries (arrows). This is easily confused with bronchial wall thickening. Note the lack of narrowing of the lumen of the bronchi. Ground glass opacity and pleural effusion are also present.
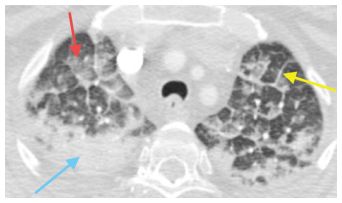
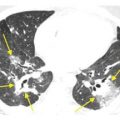
Figure 8.4
Interstitial and alveolar pulmonary edema. Smooth interlobular septal thickening (yellow arrow) is seen as a manifestation of interstitial pulmonary edema. Additionally, there is patchy bilateral ground glass opacity (red arrow) and consolidation (blue arrow) compatible with alveolar edema. Abnormalities of both interstitial and alveolar edema often coexist.
Alveolar Edema
Severe pulmonary edema results in alveolar flooding. Ground glass opacity and consolidation are the most common findings (Fig. 8.5). Ground glass opacity nodules may also be seen in a centrilobular distribution (Fig. 8.6). Findings of both interstitial and alveolar edema frequently coexist. Ground glass opacity may be associated with smooth interlobular septal or peribronchovascular interstitial thickening. A combination of ground glass opacity and interlobular septal thickening in the same lung regions, the crazy paving sign, is not uncommon (Fig. 8.7).
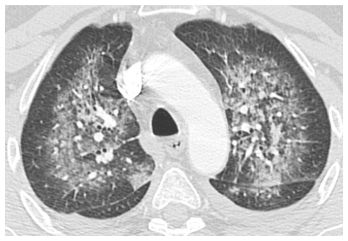
Figure 8.5
Pulmonary edema with symmetric ground glass opacity. Symmetric parahilar ground glass opacity is seen as a manifestation of pulmonary edema. Edema is classically symmetric in distribution.
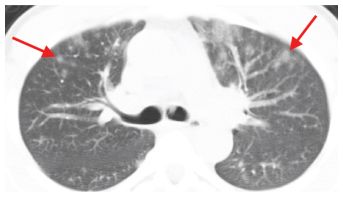
Figure 8.6
Pulmonary edema with centrilobular nodules. Ill-defined centrilobular nodules of ground glass opacity (arrows) are seen in the anterior lungs bilaterally. This is not an uncommon manifestation of edema and is often seen in association with other findings of alveolar edema.
Distribution of Hydrostatic Edema
The distribution of these abnormalities is typically diffuse or symmetric. More severe abnormalities may be seen in the dependent lung because of the normal hydrostatic gradient, but this is not always present.
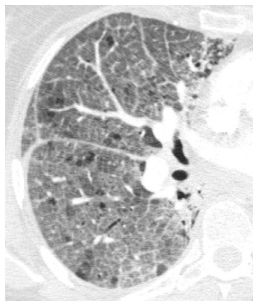
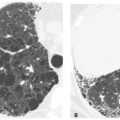
Figure 8.7
Pulmonary edema with crazy paving. A combination of ground glass opacity and smooth interlobular septal thickening is seen in the right lung. This finding is nonspecific, but pulmonary edema is one of the most common causes of this pattern in the acute setting.
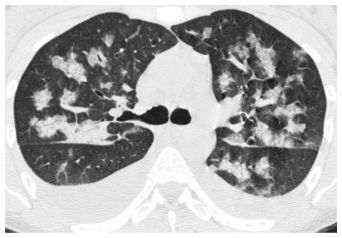
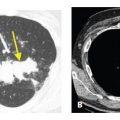
Figure 8.8
Pulmonary edema with lobular opacities. Lobular areas of ground glass opacity are present. The process is symmetric and associated with pleural effusions. Occasionally, causes of alveolar disease such as pulmonary edema may be very geographic such as in this case.
A patchy or lobular distribution of abnormalities may sometimes be present (Fig. 8.8), and in some patients, edema may be asymmetric (Fig. 8.9). Causes of asymmetric or focal pulmonary edema include the following:
1. Patient position. Pulmonary edema may occur in dependent lung regions because of gravitational effects. Patient positioning may have an influence on the location of pulmonary edema. For example, right-sided pulmonary edema may be seen in patients who lay on their right side while sleeping.
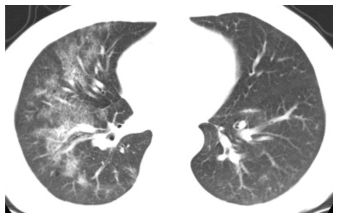
Figure 8.9
Asymmetric pulmonary edema. While edema is typically a symmetric process, unilateral or asymmetric edema is not uncommon. This patient was placed in a right side down decubitus position for a surgical procedure, explaining the unilateral right-sided edema. Patchy ground glass opacity and crazy paving are visible.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


