Stenoses → bowel obstruction with dilation of proximal bowel loops
Adhesions → angulation between adjacent loops, fixation of loops
± sinuses or fistulas (from bowel to skin, vagina, bladder, other bowel)
TOP DIFFERENTIAL DIAGNOSES
• Crohn disease
• Metastases and lymphoma
• Ischemic enteritis
• Primary bowel tumor
PATHOLOGY
• Some 20-60% of all patients with abdominal or pelvic malignancies receive radiotherapy for curative or palliative care
CLINICAL ISSUES
• Usually follows radiotherapy for primary pelvic tumors
Acute radiation enteritis or colitis often resolves spontaneously within weeks
80-90% of these will have permanent alteration of bowel habits
Moderate to severe chronic radiation enteritis/colitis develops in 5-15%
• Diagnosis is usually suggested by clinical and imaging features
Confirmed by endoscopy and biopsy if necessary
(Left) This 63-year-old man is 4 weeks status post radiation therapy for rectal cancer, now with pelvic pain and diarrhea. CT shows submucosal edema within a rigid-appearing loop of distal ileum, compatible with acute radiation enteritis.
(Right) Axial CECT in the same patient reveals numerous fluid-filled loops of proximal bowel, suggesting functional obstruction due to the radiation. The patient was treated with steroids and symptoms resolved over a 2-week period.
(Left) This 63-year-old man with a history of radiation therapy for sacral metastases, now presents with constipation. Spot film from a barium enema reveals a persistent and high-grade stricture of the rectum , typical for radiation proctitis.
(Right) Axial CECT in the same patient confirms the narrowed lumen and thickened wall of the rectosigmoid colon . Also evident is the lytic process in the sacrum , representing the metastatic focus that was the target of the radiation therapy.
TERMINOLOGY
Definitions
• Damage of small bowel or colonic mucosa and wall due to therapeutic or excessive irradiation
• Chronic radiation enteritis/colitis: Late intestinal toxicity after radiotherapy
IMAGING
General Features
• Best diagnostic clue
Mural thickening, luminal narrowing of pelvic bowel loops
• Location
Small bowel (ileum more common than jejunum)
Abdominal or pelvic colon (radiation colitis) and rectum (radiation proctitis)










 within a rigid-appearing loop of distal ileum, compatible with acute radiation enteritis.
within a rigid-appearing loop of distal ileum, compatible with acute radiation enteritis.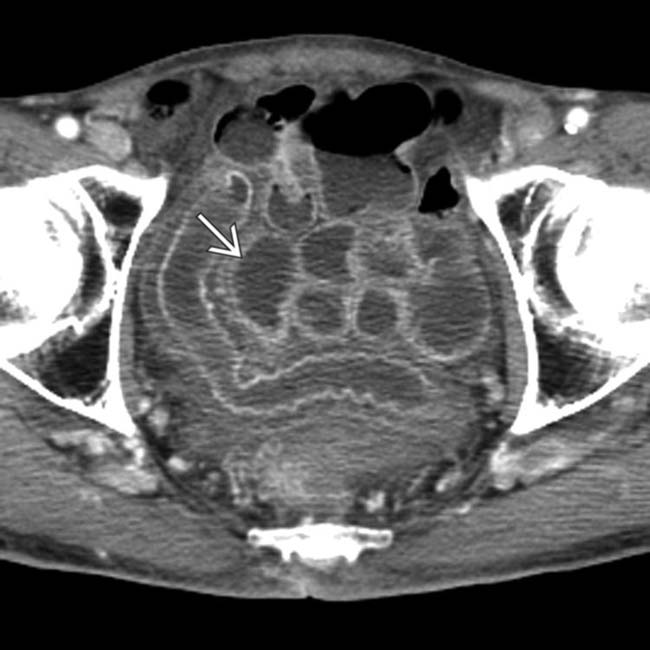
 of proximal bowel, suggesting functional obstruction due to the radiation. The patient was treated with steroids and symptoms resolved over a 2-week period.
of proximal bowel, suggesting functional obstruction due to the radiation. The patient was treated with steroids and symptoms resolved over a 2-week period.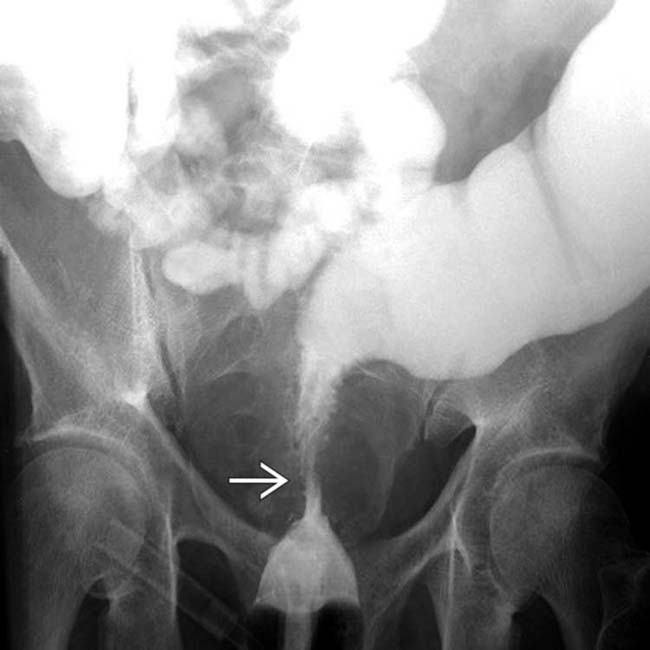
 , typical for radiation proctitis.
, typical for radiation proctitis.
 . Also evident is the lytic process in the sacrum
. Also evident is the lytic process in the sacrum  , representing the metastatic focus that was the target of the radiation therapy.
, representing the metastatic focus that was the target of the radiation therapy.













 “Target” pattern: Thickened high signal intensity submucosa surrounded by low signal intensity muscularis propria and muscularis mucosae
“Target” pattern: Thickened high signal intensity submucosa surrounded by low signal intensity muscularis propria and muscularis mucosae






