At the Second International Congress of Radiology (ICR) in Stockholm in 1928, member countries were invited to send representatives to prepare x-ray protection recommendations. The British recommendations were adopted because they were most complete; guidelines on radiation protection had been set up in that country as early as 1915.
The 1928 Congress set up the International X-Ray and Radium Protection Committee, which, after World War II, was remodeled into two commissions that survive to this day:
The International Commission on Radiological Protection (ICRP)
The International Commission on Radiation Units and Measurements (ICRU)
The US representative to the 1928 Congress was Dr. Lauristor Taylor who brought back to the United States the agreed radiation protection criteria and set up a national committee, the Advisory Committee on X-Ray and Radium Protection, under the auspices of the Bureau of Standards, which was perceived to be a “neutral territory” by the various radiologic societies of the day; this committee operated until World War II. In 1946, it was renamed the National Council on Radiation Protection and Measurements (NCRP), eventually receiving a charter from Congress as an independent body to provide advice and recommendations on matters pertaining to radiation protection in the United States. NCRP reports still form the basis of radiation protection policy in the United States today, although legal responsibility for the implementation of radiation safety is variously in the hands of the Nuclear Regulatory Commission (NRC), the Department of Energy (DOE), and state or city bureaus of radiation control.
▪ ORGANIZATIONS
The organization of radiation protection and the interrelation of the various committees, whose reports are quoted, deserve a brief explanation.
First, there are the committees that summarize and analyze data and suggest risk estimates for radiation-induced cancer and heritable effects. At the international level, there is the United Nations Scientific Committee on the Effects of Atomic Radiation, usually known as UNSCEAR. This committee has wide international representation, being composed of scientists from 21 member states. Comprehensive reports appeared at intervals over the years since 1958, with the latest report in 2000. The United States committee is appointed by the National Academy of Sciences and is now known as the Biological Effects of Ionizing Radiations (BEIR) Committee. The first report appeared in 1956, when it was known as the Biological Effects of Atomic Radiations (BEAR) Committee. Subsequent comprehensive reports appeared in 1972 (BEIR II), 1980 (BEIR III), 1990 (BEIR V), and 2006 (BEIR VII). BEIR VI, entitled The Health Effects of Exposure to Indoor Radon, appeared in 1999.
These committees are “scholarly” committees in the sense that if information is not available on a particular topic, they do not feel compelled to make a recommendation. Because they do not serve an immediate pragmatic aim, they are not obliged to make a “best guess” estimate if data are uncertain.
Second, there are the committees that formulate the concepts for use in radiation protection and recommend maximum permissible levels. These committees serve more pragmatic aims and, therefore, must make best estimates even if good data are unavailable. At the international level, there is the ICRP, which, together with ICRU, was established in 1928 after a decision by the Second ICR, as mentioned earlier. In 1950, the ICRP was restructured and given its present name. The ICRP often takes the lead in formulating concepts in radiation protection and in recommending dose limits. As an international body, it has no jurisdiction over anyone and can do no more than recommend; it has established considerable credibility, however, and its views carry great weight. Its most recent comprehensive report is ICRP Publication No. 103, published in 2007. The United Kingdom, most of Europe, and Canada follow ICRP recommendations. In the United States, there is the NCRP (also mentioned earlier) chartered by Congress to be an “impartial” watchdog and consisting of 100 experts from the radiation sciences—who are, therefore, not impartial at all. The NCRP often, but not always, follows the lead of ICRP. Their most recent comprehensive report on dose limits (NCRP Report No. 116, published in 1992) differs from ICRP in several important respects. The ICRP and NCRP suggest dose limits and safe practices but, in fact, neither body has any jurisdiction to enforce their recommendations.
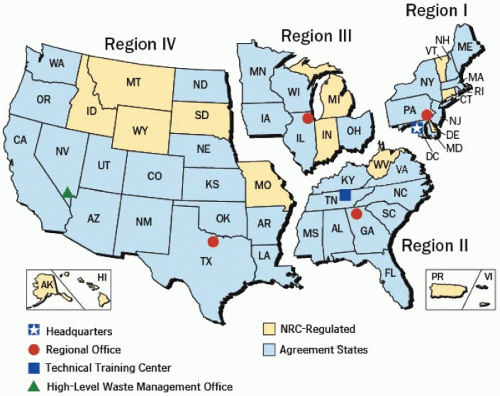
FIGURE 17.1 The NRC formulates rules for radioactive by-product material from reactors in “agreement states.” The figure shows agreement states as of 2009.
In the United States, the Environmental Protection Agency (EPA) has the responsibility for providing guidance to federal agencies; it is the EPA that sets, for example, the action level for radon. Each state can formulate its own regulations for x-rays and radiations produced by sources other than reactors. In agreement states, the NRC formulates rules for by-product materials from reactors. Figure 17.1 shows the agreement status as of 2009. In other states, this responsibility falls on the U.S. Department of Labor Occupational Safety and Health Administration (OSHA). The DOE is responsible for radiation safety regulations at all of its facilities operated by contractors. Up to the present, the various regulating bodies in the United States have accepted, endorsed, and used the reports issued by the NCRP, but they are not obliged to do so, and they are often slow to adopt the latest reports.
▪ QUANTITIES AND UNITS
Dose
The quantity used to measure the “amount” of ionizing radiation is the absorbed dose, usually termed simply as dose. This is defined as the energy absorbed per unit mass, and its unit is joules per kilogram, which is given a special name, the gray (Gy), named after the British physicist who contributed to the development of ionization chamber theory. The unit used in the past was the radiation absorbed dose (rad), defined as an energy absorption of 100 erg/g. Consequently, 1 Gy equals 100 rad.
Radiation Weighting Factor
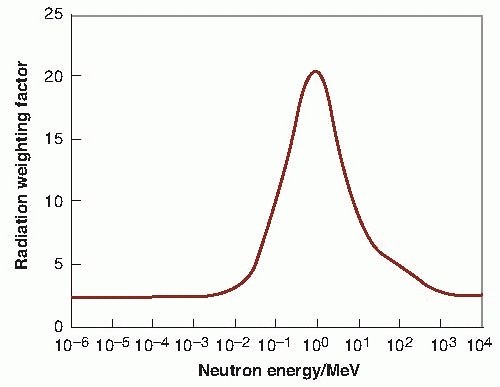
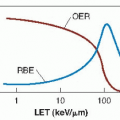
The probability of a stochastic effect, such as the induction of cancer or of heritable events, depends not only on the dose, but also on the type and energy of the radiation; that is, some radiations are biologically more effective for a given dose than others. This is taken into account by weighting the absorbed dose by a factor related to the quality of the radiation. A radiation weighting factor (WR) is a dimensionless multiplier used to place biologic effects (risks) from exposure to different types of radiation on a common scale. The WRs are chosen by the ICRP as representative of relative biologic effectiveness (RBE) applicable to low doses and low dose rates (LDR), and for biologic end points relevant to stochastic late effects. They can be traced ultimately to experimentally determined RBE values, but a large judgmental factor is involved in their choice. The weighting factors recommended by the ICRP for photons, electrons, protons and α-particles, and heavy ions are shown in Table 17.1. For neutrons, a continuous curve as a function of neutron energy is recommended (Fig. 17.2) with the most biologically effective neutrons having a WR of 20.
A continuous curve as a function of neutron energy
a All values relate to the radiation incident on the body or, for internal sources, emitted from the source.
From ICRP 2007.
Equivalent Dose
In radiologic protection, the equivalent dose is the product of the absorbed dose averaged over the tissue or organ and the WR selected for the type and energy of radiation involved. Thus:
If absorbed dose is measured in Gy, the equivalent dose is measured in sievert (Sv), named after the Swedish physicist who designed early ionization chambers. Although 1 Gy of neutrons does not produce the same biologic effect as 1 Gy of x-rays, 1 Sv of either neutrons or x-rays does result in equal biologic effects. The ICRP has recommended a new name for this quantity: radiation weighted dose. The commission is also considering a new (special) name for the unit of radiation weighted dose so as to avoid the use of “sievert” for both radiation weighted dose and effective dose.
FIGURE 17.2 WR for neutrons as a function of neutron energy. (From the ICRP 2007 recommendations.)
If a radiation field is made up of a mixture of radiations, the equivalent dose is the sum of the individual doses of the various types of radiations, each multiplied by the appropriate WR. Thus, if a tissue or organ were exposed to 0.15 Gy of cobalt-60 γ-rays plus 0.02 Gy of 1-MeV neutrons, the equivalent dose would be:
Effective Dose
If the body is uniformly irradiated, the probability of the occurrence of stochastic effects (cancer and hereditary effects) is assumed to be proportional to the equivalent dose, and the risk can be represented by a single value. In fact, truly uniform total body exposures are rare, particularly if irradiation is from radionuclides deposited in tissues and organs. Sometimes, equivalent doses to various tissues differ substantially and it is well established that different tissues vary in their sensitivities to radiation-induced stochastic effects. For example, it is difficult to produce heritable effects by irradiation of the head or hands. On the other hand, the thyroid and breast appear to be particularly susceptible to radiation-induced cancer. To deal with this situation, the ICRP introduced the concept of the tissue weighting factor (WT), which represents the relative contribution of each tissue or organ to the total detriment resulting from uniform irradiation of the whole body. Table 17.2 lists the WT values recommended by the ICRP in 2007.
The sum of all of the weighted equivalent doses in all the tissues or organs irradiated is called the effective dose, which is expressed by the formula
for all tissues or organs exposed. Effective dose is in principle, as well as in practice, a nonmeasurable quantity.
Committed Equivalent Dose
In the case of external irradiation, the absorbed dose is delivered at the time of exposure; but for irradiation from internally deposited radionuclides, the total absorbed dose is distributed over time as well as to different tissues in the body. The dose rate falls off depending on the physical and biologic half-lives of the radionuclide.
To take into account the varying time distributions of dose delivery, the ICRP defined the committed equivalent dose as the integral over 50 years of the equivalent dose in a given tissue after intake of a radionuclide. This time was chosen to correspond to the working life of a person. For radionuclides with effective half-lives of up to about 3 months, the committed equivalent dose is essentially equal to the annual equivalent dose in the year of intake; but for radionuclides with longer effective half-lives, it is greater because it reflects the dose that will accrue over future years.
TABLE 17.2 Tissue Weighting Factors
Organ/Tissue
Number of tissues
wT
Total contribution
Lung, stomach, colon, bone marrow, breast, and remainder
6
0.12
0.72
Gonads
1
0.08
0.08
Thyroid, esophagus, bladder, and liver
4
0.04
0.16
Bone surface, skin, brain, and salivary glands
4
0.01
0.04
The specified remainder tissues (14 in total, 13 in each sex) are adrenals, extrathoracic tissue (ET), gall bladder, heart, kidneys, lymphatic nodes, muscle, oral mucosa, pancreas, prostate (m), small intestine (SI), spleen, thymus, uterus/cervix (f).
From ICRP 2007.
Committed Effective Dose
If the committed equivalent doses to individual organs or tissues resulting from the intake of a radionuclide are multiplied by the appropriate WT and then summed, the result is the committed effective dose.
Collective Equivalent Dose
The quantities referred to previously all relate to the exposure of an individual. They become appropriate for application to the exposure of a group or population by the addition of the term collective. Thus, the collective equivalent dose is the product of the average equivalent dose to a population and the number of persons exposed. There appears to be some confusion about the accepted name of the unit for collective equivalent dose in the new SI system of units. Some use man-sievert, presumably agreeing with the judgment of Sir Winston Churchill that “man embraces woman.” The more liberated prefer the term person-sievert, which is used here.
Collective Effective Dose
The collective effective dose is likewise the product of the average effective dose to a population and the number of persons exposed. The unit is again the person-sievert. An example is in order here. If 100 persons receive an average effective dose of 0.3 Sv, the collective effective dose is 30 person-Sv.
Collective Committed Effective Dose
In the case of a population ingesting or inhaling radionuclides that deposit their dose over a prolonged period, the integral of the effective dose over the entire population out to a period of 50 years is called the collective committed effective dose.
These collective quantities can be thought of as representing the total consequences of exposure of a population or group and they can be thought of as surrogates for “harm.” For example, the annual collective effective dose to the US population from medical radiation is about 899,000 person-Sv. Such collective quantities are much beloved by the bureaucrats because they make it possible to compare different activities or accidents, inasmuch as each can be described by a single number. The danger is that the next step is to convert the collective dose into the number of cancers or heritable effects produced, which, of course, assumes proportionality between dose and biologic effect, which is seldom true. The quantities certainly are used widely to give a rough guide to the probability of cancer and heritable effects in a population exposed to radiation, and in particular, they can be used to compare the approximate impact of different types of radiation accidents in terms of several health effects that might arise in that population.
Summary of Quantities and Units
Table 17.3 is a summary of the quantities and units that have been described here, showing how they build logically on one another. If on reading this section the reader gains the impression that the bureaucrats have taken over, it is because they have—at least in the field of radiation protection. An elaborate set of definitions has been produced based on the assumption of linearity between dose and risk. The whole business needs to be taken with a generous grain of salt because it is like a house of cards, based on somewhat shaky premises.
TABLE 17.3 Quantities and Units Used in Radiation Protection
Quantity
Definition
Unit
Absorbed dose
Energy per unit mass
Gray
For individuals
Equivalent dose (radiation weighted dose)
Average dose × radiation weighting factor
Sievert
Effective dose
Sum of equivalent doses to organs and tissues exposed, each multiplied by the appropriate tissue weighting factor
Sievert
Committed equivalent dose
Equivalent dose integrated over 50 years (relevant to incorporated radionuclides)
Sievert
Committed effective dose
Effective dose integrated over 50 years (relevant to incorporated radionuclides)
Sievert
For populations
Collective effective dose
Product of the average effective dose and the number of individuals exposed
Person-sievert
Collective committed effective dose
Integration of the collective dose over 50 years (relevant to incorporated radionuclides)
Person-sievert
The concept of collective effective dose does allow a rough and quick estimate to be made of the potential health hazards to a population from, for example, an accidental release of radioactivity from a nuclear reactor. It must be emphasized again that these concepts can be used only under conditions in which it is reasonable to assume linearity between risk and dose— that is, that risks are directly proportional to the summation of doses from different sources. Exposures that are within the administratively allowed dose limits may cause an increased incidence of stochastic effects, such as cancer and heritable effects, but are much below the thresholds for early deterministic effects. In the case of larger accidental releases in which doses to some people might be high enough to exceed these thresholds to the point of causing early death, collective effective dose is an inappropriate quantity.
▪ AIMS AND OBJECTIVES OF RADIATION PROTECTION
The fundamental aim of radiation protection has been summed up by the ICRP as follows:
The primary aim of radiologic protection is to provide an appropriate standard of protection for man without unduly limiting the beneficial actions giving rise to radiation exposure. This aim cannot be achieved based on scientific concepts alone. All those concerned with radiologic protection have to make value judgments about the relative importance of different kinds of risk and about the balancing of risks and benefits. In this, they are no different from those working in other fields concerned with the control of hazards.
As stated by the NCRP, the objectives of radiation protection are the following:
To prevent clinically significant radiationinduced deterministic effects by adhering to dose limits that are below the apparent or practical threshold, and
To limit the risk of stochastic effects (cancer and heritable effects) to a reasonable level in relation to societal needs, values, and benefits gained.
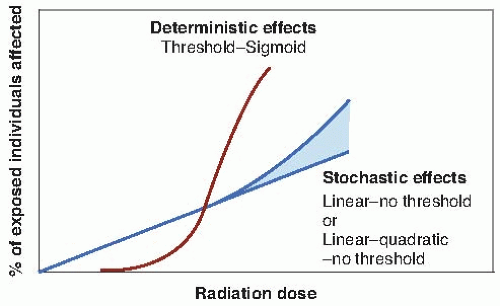
FIGURE 17.3 The basic differences in the shape of the dose-response relationship for stochastic as opposed to deterministic effects. Deterministic effects (e.g., cataracts or mental retardation) show a threshold in dose; the severity of the effect increases with dose above this threshold, and the proportion of individuals rises rapidly with dose to 100%. The dose-response relationship is, therefore, sigmoid after a threshold. Stochastic effects are all-ornothing effects (e.g., cancer and heritable effects). The severity of the effect is not dose related, although the probability of it occurring is. The increase with dose may be linear or linear-quadratic. There is no threshold, that is, no dose below which the probability of an effect is zero. The dose-response relationship is, therefore, linear or linear-quadratic, with no threshold.
The difference in shape of the dose-response relationships for deterministic and stochastic effects is illustrated in Figure 17.3. The objectives of radiation protection can be achieved by reducing all exposure to as low as reasonably achievable (ALARA) and by applying dose limits for controlling occupational and general public exposures. For radiation protection purposes, it is assumed that the risk of stochastic effects is strictly proportional to dose without threshold throughout the range of dose and dose rates of importance in radiation protection. Furthermore, the probability of response (risk) is assumed to accumulate linearly with dose. This is not true at higher doses characteristic of radiation accidents in which more complex (nonlinear) dose-risk relationships may apply.
Given these assumptions, any selected dose limit has an associated level of risk. Consequently, it is necessary to justify any use of radiation in terms of a benefit to a person or to society.
Justification of exposure is one of the basic principles of radiation protection. The concept was described in 1977 by the ICRP: A practice involving exposure to radiation should produce sufficient benefit to the exposed individual or to society to offset the radiation detriment it causes. This concept is sometimes difficult to put into practice in various situations in which individuals are exposed as follows:
In the case of patients, the diagnostic or therapeutic benefit should outweigh the risk of detriment.
In the case of occupational exposure, the radiation risk must be added to and compared with other risks in the workplace.
The most difficult situation is exposure for the sake of research, where volunteer subjects may fall into one of three categories: Patients who may benefit, patients who may receive no benefit, and healthy volunteers. In cases in which the individual receives no benefit, the benefit to society must outweigh the risks.
▪ BASIS FOR EXPOSURE LIMITS
Exposure limits have changed over the years in step with evolving information about the biologic effects of radiation and with changes in the social philosophy within which recommended exposure limits are developed.
In the 1930s, the concept of a tolerance dose was used, a dose to which workers could be exposed continuously without any evident deleterious acute effects such as erythema of the skin.
By the early 1950s, the emphasis had shifted to late effects. The maximum permissible dose (MPD) was designed to ensure that the probability of the occurrence of injuries was so low that the risk would be readily acceptable to the average person. At about that time, based on the results of genetic studies in Drosophila and mice, the occupational limit was reduced substantially and a limit for exposure of the public introduced. Subsequently, the heritable effects were found to be smaller, and cancer risks larger than were thought at the time.
By the 1980s, the NCRP was comparing the probability of radiation-induced cancer death in radiation workers with annual accidental mortality rates in “safe” industries. Exposure standards, therefore, are necessarily based partly on observed effects, but with a great deal of judgment involved.
Earlier chapters described the deleterious effects of radiation in terms of heritable effects, carcinogenesis, and effects on the developing embryo and fetus. The risk estimates derived are summarized in Table 17.4. By far, the largest risk estimate is 40% per Sv for severe mental retardation for the most sensitive period of gestation and above a threshold of at least 0.3 Gy. Next comes carcinogenesis as 5% per Sv, corresponding to exposure of the general population to low doses and dose rates. Last are heritable effects, lowered in 2004 by the ICRP to 0.2% per Sv for the general population.
Only gold members can continue reading. Log In or Register to continue