This article focuses on the variety of imaging features of paravertebral ossifications that are of practical interest in the diagnosis of diseases. The spinal anatomy is reviewed and correlated to paravertebral ligamentous ossifications and their potential clinical impact. A vertebral bony outgrowth is secondary to inflammation or degeneration and can be characterized based on its origin and growth direction, in addition to appreciation of intervertebral disc space preservation or loss. Imaging in rheumatology patients is highlighted because early detection of disease is of increasing importance. A correlation between radiographs and MR imaging is made.
Key points
- •
Calcifications and ossifications of paravertebral ligaments may cause clinical symptoms.
- •
Differentiation between hypertrophied ligaments and ligamentous calcifications is limited using MR imaging alone.
- •
A vertebral bony outgrowth can be characterized on radiographs based on its origin and growth direction.
- •
A suspected axial spondyloarthritis on radiograph or MR imaging of the spine can be followed by MR imaging of the sacroiliac joints for definite diagnosis.
- •
There is a high prevalence of degenerative changes in the spine, seen as early as the age of 16 years, without clinical significance.
Introduction
Radiographs have been the cornerstone in diagnostic imaging. In the case of back pain, a common complaint in the general population, conventional imaging of the spine is still one of the first imaging methods performed. However, there is a high prevalence of degenerative changes in the spine, described in up to 70% in a young population without clinical significance. These findings will increase with age. Inflammatory back pain, on the other hand, is only present in a minority of patients, and specific imaging findings should raise the suspicion of spondyloarthritis. The availability of effective medication in rheumatology has shifted the attention toward early disease detection. MR imaging is the only imaging modality to detect bone marrow edema, and its role has become more important. Because MR imaging–detected sacroiliitis is part of the Assessment of SpondyloArthritis International Society (ASAS) criteria for the classification of patients at an early stage, MR imaging is increasingly used. Here, attention is paid to radiographs and MR imaging of the spine, more specifically, to the variety of imaging features of paravertebral ossifications. Certain types of ossifications can be diagnostic for a disease, and others are merely correlated to aging. Therefore, correct interpretation is clinically important. These paravertebral ossifications can be primarily ligamentous or bony in origin. Differentiation between these two origins is not always possible and not always necessary if some general guidelines in interpretation are used. Because both radiographs and MR imaging of the spine are widely performed, knowledge of a correlation between these two imaging modalities might be useful in clinical practice.
Therefore, the purpose of this article is to review the anatomy of the spine, to describe paravertebral ligamentous ossifications, to understand the development of vertebral bony outgrowths and correlate these to specific diseases, and finally, to correlate radiographic and MR imaging findings in paravertebral ossifications.
Anatomy of the discovertebral junction
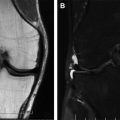
The intervertebral disc consists of an outer layer, the annulus fibrosus, and a slightly posteriorly located central zone, the nucleus pulposus. In the superior and inferior endplates of the vertebral body is a central depression covered with cartilage, the fused epiphyseal rings form the periphery. The annulus fibrosus is attached to the vertebral endplate by strong fibers. The external fibers, Sharpey fibers, penetrate the outer bony ring. These fibers also extend beyond the confines of the disc and blend with the vertebral periosteum and anterior longitudinal ligament ( Fig. 1 ).

Anatomy of the spinal ligaments
The anterior longitudinal ligament is a broad fibrous band located at the anterior part of the vertebral column, extending from skull to sacrum (see Fig. 1 ; Fig. 2 ). The posterior longitudinal ligament is a thinner band of fibers at the posterior vertebral column, located within the spinal canal anteriorly. It extends from the level of the axis and membrana tectoria to the sacrum. Both anterior and posterior longitudinal ligaments are attached to the margins of the vertebral bodies and loosely attached to the intervertebral discs. Whereas the anterior longitudinal ligament is adherent to the anterior surface of the vertebral body, the posterior longitudinal ligament forms a bow stretching over the concave posterior surface. The ligamenta flava form the posterior ligamentous demarcation of the spinal canal. They are attached to the articular capsule of the apophyseal joints, connect the laminae, and meet in the midline. These ligaments increase in thickness from cranial to caudal. The interspinal ligaments interconnect the spinous process to each other, and the intertransverse ligaments extend between the transverse processes of the vertebrae. The ligamentum nuchae extends from the external occipital protuberance to C7. Below C7 extending to the sacrum, the supraspinal ligament connects the tips of the spinous processes.

Normal aging
The pediatric spine changes in appearances with aging, and ossification centers and synchondroses may be multiple and variable. The normal appearance and fusion of the superior and inferior ring apophysis for different pediatric age groups have recently been reported. An ununited secondary ossification center (limbus vertebra) is a normal variation, which is suggested to be the result of intervertebral disc herniation.
When we age, the nucleus pulposus decreases its water content; the mucoid matrix is replaced by fibrocartilage, and it will resemble the annulus fibrosus. The discs will lose their height. Calcifications or ossifications of spinal ligaments are part of normal aging and a physiologic process.
Part 1
Paravertebral Ligamentous Ossifications
Ligamentous ossifications may become more prominent in time, and these are most frequently seen in the anterior longitudinal ligament as part of diffuse idiopathic skeletal hyperostosis (DISH). These ossifications are often asymptomatic and diagnosed on radiographs; however, specific criteria do exist and need to be met (see later discussion). Posterior spinal ligaments may ossify as well, and their close proximity to the spinal canal may cause neurologic symptoms. Diagnosing posterior ossifications on radiographs might be challenging because of overlying osseous structures, and computed tomography (CT) is used to confirm ossification. MR imaging is of additional value in the case of neurologic symptoms to evaluate spinal cord compression. A limitation of MR imaging is that differentiation between hypertrophy of ligaments and calcifications is difficult. Ligaments and calcifications are both low of signal intensity on T1-weighted and T2-weighted fat-saturated images. Ossifications can be confirmed in the presence of fatty marrow, which are of high signal intensity on T1-weighted images and suppressed on T2-weighted fat-saturated images. Because of the small size of ligamentous ossifications and their potential impact, CT can be used for further investigation. Exceptions with extensive paraspinal ligament ossifications occur.
Anterior Longitudinal Ligament and Soft Tissues
Diffuse idiopathic skeletal hyperostosis
DISH is a skeletal disorder, with typical changes in the spine as well as extraspinal involvement. Because this disease is characterized in part by calcification and ossification of the anterior longitudinal ligament, this is discussed here. The extraspinal locations include hyperostosis at ligament insertions, usually the pelvis, calcaneus, tarsal bones, ulnar olecranon, and patella. It has often been referred to as Forestier disease. DISH is a common entity, affecting middle-aged and elderly patients, predominantly men. Its origin is unknown. It may be asymptomatic or associated with mild to moderate restriction of motion. It is suggested that certain symptoms and signs, including stiffness, range of motion, and tendinosis, are part of the disease spectrum, consistent with radiographic and radionuclide findings.
Radiographic criteria
The 3 following radiographic diagnostic criteria are defined for the definite diagnosis of DISH:
- 1.
Flowing calcification and ossification along the anterolateral aspects of at least 4 contiguous vertebra.
- 2.
A relative normal intervertebral disc space at these levels, without characteristics of degenerative disc disease, including vacuum phenomena and vertebral body marginal sclerosis.
- 3.
Absence of apophyseal joint bony ankylosis and sacroiliac joint erosion, sclerosis, or bony fusion ( Figs. 3 and 4 ).

Fig. 3
DISH of the thoracic spine, PA ( A ) and lateral ( B ), in a 62-year-old man. Excessive flowing ossifications at the anterolateral spine on more than 4 levels. The left site is thought to be less involved secondary to aortic pulsations.

Fig. 4
Cervical spine radiograph ( A ) anteroposterior (AP) and ( B ) lateral view of a 63-year-old man. Bony outgrowths at the anterior margin of the vertebra, predominantly extending from the anterior endplate distally, characteristic of DISH. The intervertebral disc spaces are preserved.
These criteria help to differentiate from the following:
- 1.
Spondylosis deformans,
- 2.
Intervertebral osteochondrosis, degenerative disc disease, and
- 3.
Ankylosing spondylitis.
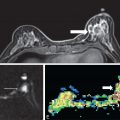
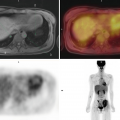
A recent systematic review article shows that different classification criteria for DISH are available, and that there is a lack of consensus on the (early) diagnosis. Hyperostosis is gradually formed at the anterior vertebral body, appearing at the anterior margin and extending downwards (see Figs. 3 and 4 ). The flowing ossification may show a radiolucent disc extension at the intervertebral level, with a small ossicle anterior tot the disc space. Such an appearance is less frequently seen in the cervical spine than in the thoracic spine. CT might help to exclude a fracture ( Fig. 5 ). DISH at the cervical spine may cause dysphagia owing to large ossifications, which are diagnosed on conventional imaging. It should be noted that in the cervical spine concomitant posterior vertebral abnormalities are not infrequent, including ossification of the posterior longitudinal ligament (OPLL) as well as hyperostosis of the posterior vertebral body and osteophytes. A patient with DISH may show activity on a radionuclide study ( Fig. 6 ). Involvement of the atlantoaxial level may show a crowned dens and can be extensive in some cases ( Fig. 7 ). In DISH, the role of MR imaging is limited, unless additional posterior spine involvement is causing neurologic complaints. Because in early stages disease activity on MR imaging might be visualized at the enthesis, looking at early radiographic changes may lead to the correct diagnosis.



Acute calcific tendinitis of the longus colli muscle
On normal conventional imaging of the lateral cervical spine, the anterior prevertebral soft tissues are closely approximated to the anterior vertebral bodies from C1-4. The anterior longitudinal ligament and the longus colli muscle form this 3- to 4-mm soft tissue shadow. A widened prevertebral space C1-4 is abnormal and reason for further clinical and radiological investigation. In a clinical presentation of progressive severe pain in the cervical spine and subfebrile temperature, a retropharyngeal abscess is in the differential diagnosis. However, (subtle) prevertebral calcifications should raise the diagnosis of acute calcific tendinitis of the longus colli muscle ( Figs. 8 and 9 ), an aseptic inflammatory response to deposition of calcium hydroxyapatite in the longus colli muscle tendons ( Fig. 10 ). On MR imaging, inhomogeneous enhancing prevertebral soft tissues are visualized. The calcific deposition is of low signal intensity on all sequences and not enhancing and should not be misinterpreted as an abscess. Calcifications either on conventional radiograph or on additional CT are diagnostic for acute calcific tendinitis of the longus colli muscle/retropharyngeal tendinitis. Typically, the superior oblique fibers of the longus colli muscle are involved, extending from the anterior atlas to anterior tubercles of the transverse processes C3-5 (see Fig. 10 ).



Conservative treatment includes the use of nonsteroidal anti-inflammatory drugs (NSAIDs). The specific location and clinical information differentiate this from enthesitis in spondylarthropathy (see later discussion).
Posterior Ligaments and Soft Tissues
Ossification of ligaments in the periphery of the spinal canal may decrease the subarachnoid space, leading to acquired spinal stenosis and neurologic symptoms and signs.
Calcification or ossification of the posterior longitudinal ligament
OPLL and the association with progressive cervical myelopathy in a Japanese patient were first published in 1960. Its prevalence has been investigated in Japan, and among patients with cervical spine disorders on conventional radiographs, it varies between 1% and 1.7%. Among asymptomatic Japanese patients older than 30 years of age, it is reported to be 1.9% to 4.3%. In non-Japanese patients, a much lower prevalence of 0.1% to 1.7% is described. An explanation for the probably of higher incidence of symptomatic patients in Japan may be the associated narrowing of the spinal canal. Its cause is uncertain. It has been reported in patients with DISH and ankylosing spondylitis. It is most commonly seen in the midcervical region. The thoracic and lumbar spine is involved in about 20% of cases; of these, the fourth to seventh thoracic level is most frequently affected ( Figs. 11–14 ). OPLL is more frequent in men than in women and may be asymptomatic ( Fig. 15 ). Neurologic symptoms and signs can be initiated by trauma.