This article covers the use of radiographs and MR imaging for diagnosing elbow disorders. It concentrates on these techniques, but other imaging techniques including computed tomography, ultrasound, and nuclear medicine are discussed when clinically important. The article covers the use of imaging for specific symptoms including lateral, medial, anterior, posterior and generalized elbow pain, focal swelling, restriction of movement, locking, and neurologic symptoms. Radiographs have been the mainstay of initial imaging of the elbow, while ultrasound examination is often used for soft tissue disease. MR imaging has the advantage over radiographs and ultrasound in accurately examining bone and soft tissue together.
Key points
- •
Radiographs are the mainstay of elbow imaging in trauma.
- •
Soft tissue disorders are common around the elbow, but radiographs are rarely helpful.
- •
MR imaging can be used to interrogate the soft tissues and bone.
Introduction
The emphasis of this article is on the use of radiographs and MR imaging for the diagnosis of elbow disorders. For completeness, the authors have included discussion relating to other imaging techniques, including computed tomography (CT), ultrasound, and nuclear medicine where they are of clinical importance.
Radiographs have been the mainstay of initial imaging of the elbow, particularly in the trauma setting. In the absence of traumatic injury, most of the disease processes encountered in the elbow relate to the soft tissues. Ultrasound examination will then be performed prior to radiographs when soft tissue disease is suspected. MR imaging has the advantage over radiographs and ultrasound in accurately examining both bone and soft tissue.
This article concentrates on the use of radiographs and MR imaging when the patient presents with particular symptoms. Fractures and children’s abnormalities are covered in other articles.
General
Radiographs
Value
The value of conventional radiographs is that they typically clearly show fractures if at least 2 views of the affected area are undertaken. Furthermore, they are used in the initial assessment of bone pain as an examination to exclude bone tumors. They will demonstrate areas of lysis, calcification, and sclerosis within the bone. Bone textual changes may be observed including cortical scalloping and disturbance of the trabecular pattern of the medulla. Irregularity of the cortex may be seen in the enthesitis at the site of tendon insertion.
Displacement of fat pads in the soft tissues will identify larger joint effusions. Swollen soft tissues and calcification within the soft tissue may be observed. Fat-containing mass lesions may be seen as a radiolucent area within the soft tissue.
Limitations
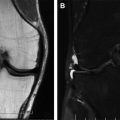
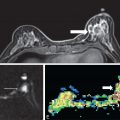
A major limitation of conventional radiographs is that they are only a 2-dimensional image of a 3-dimensional object, and therefore abnormalities may be obscured by the overlying tissue. Microfracturing of bone will not be identified, and at least 80% of the bone must be destroyed before a radiograph will show a lucency when the destruction is centrally located. When there is cortical destruction, this will be identified sooner. This means that radiographs will not detect many cases of early cancer ( Figs. 1 and 2 ).


In addition, the contrast between different soft tissue types is low, thus reducing the sensitivity of diagnosis, meaning many soft tissue abnormalities cannot be identified by radiographs.
MR Imaging
MR imaging will clearly show abnormality within the bone such as microfracturing, a bone tumor, or enthesitis. This of course depends on the correct sequences being performed-to optimize the conspicuity of bone lesions. T1 spin echo and short T1 inversion recovery (STIR) sequence should be performed. The use of T1 fast spin echo, proton density fat saturation, and T2 gradient echo sequences can obscure some bone lesions.
MR imaging will clearly identify abnormalities of the soft tissue when using the appropriate sequences. The tendons, ligaments, muscles, nerves, vessels, and subcutaneous soft tissue can be interrogated in detail.
The authors discuss the use of radiographs and MR imaging in the following clinical settings:
- •
Lateral elbow pain
- •
Medial elbow pain
- •
Anterior elbow pain
- •
Posterior elbow pain
- •
Generalised elbow pain
- •
A focal swelling
- •
Restriction of motion
- •
Locking
- •
Forearm and hand neurological symptoms
Lateral elbow pain
The causes of lateral elbow pain are given in Box 1 .
Common
Extensor tendinopathy (activity related)
Referred pain (prolonged posture)
- •
Cervical spine
- •
Upper thoracic spine
- •
Neuromyofascial
- •
Less common
Radiocapitellar joint synovitis, osteoarthritis
Posterior interosseous nerve entrapment
Lateral collateral ligament injury
Not to be missed
Osteochondritis dissecans
When a patient presents with pain on the radial side of the elbow, a radiograph is the initial investigation to exclude osteoarthritis of the radiocapitellar joint. This will be identified by the features including the presence of marginal osteophytes, irregular joint space narrowing, subchondral sclerosis, and subchondral cysts. In younger patients, there may be osteochondritis dissecans of the capitellum.
Calcification may be visible on the radiograph along the lateral epicondyle secondary to enthesitis. Please note that the presence of calcification is not limited to enthesitis; it can also be seen in soft tissue masses, including tumors and myositis ossificans and due to be calcification in an abnormal tendon ( Fig. 3 ).

MR imaging may detect more subtle radiocapitellar osteoarthritis where there is cartilage loss and subchondral edema. The pseudodefect of the capitellum must be appreciated in the younger patient, and this can be misdiagnosed as an osteochondral fracture.
The pain may arise from the lateral tendon insertions. The most commonly affected tendon group is the common extensor origin (CEO), commonly called tennis elbow or lateral epicondylitis.
On MR imaging, the extensor digitorum communis, extensor digiti minimi, and extensor carpi radialis brevis tendons have a common origin on the superior aspect of the lateral epicondyle. On the posterior inferior aspect of the lateral epicondyle is the insertion of the extensor carpi ulnaris, and this is separated from the insertion of the anconeus by fat.
The common insertion of the radial collateral ligament and lateral ulnar collateral ligament on the superior aspect of the intertubercular sulcus and inferior aspect of the superior tubercle may also be identified.
Common extensor tendinosis occurs in patients who perform repeated extension of their wrists with gripping and supination. It is seen in novice tennis players because of poor backhand technique rather than in elite competitors (tennis elbow is never seen at Wimbledon). Interestingly, it is also more commonly seen in golfers than golfers’ elbow and is reported in around 85% of golfers. In golfers, the left elbow is affected in right-handed players and vice versa. The disease commences at the origin of the extensor carpi radialis brevis and as the disease progresses, tearing of the undersurface of this tendon occurs. This can sometimes lead to a more extensive tearing over time. This abnormality will be clearly seen by MR imaging but not on a radiograph. On an MR imaging fluid-sensitive sequence, the area of abnormality will be of high signal intensity because of mucoid degeneration of the tendon and/or tearing with fluid in the gap. If calcification is present, this will typically be of low signal on all sequences. There may be associated edema within the anconeus muscle. The anconeus muscle is thought to be a lateral stabilizer of the elbow blending with the lateral joint capsule and lateral triceps muscle. Avulsion injuries isolated to this muscle can therefore also be seen. MR signal changes within the CEO can be seen following a recent injection and in the asymptomatic patient; hence clinical correlation is advised.
The lateral collateral ligament is commonly thickened or torn when there is an extensive common extensor origin tendinosis, as it blends with the undersurface of the tendons.
Medial elbow pain
The causes of medial elbow pain are given in Box 2 .
Common
Flexor tendinopathy (activity related)
Medial collateral ligament sprain
Less common
Ulnar nerve compression
Avulsion fracture of medial epicondyle (adolescents)
Apophysitis (adolescents)
Not to be missed
Referred pain (prolonged posture)
- •
Cervical spine
- •
Upper thoracic spine
- •
Neuromyofascial
- •
Established osteoarthritis of the medial humeroulnar joint will be detected on radiographs by the same features as described for lateral elbow pain.
MR imaging may detect more subtle medial osteoarthritis when there is cartilage loss and subchondral edema. The pseudodefect of the trochlear transverse ridge is a pitfall in MR imaging interpretation.
Approximately 9.8% to 20% of epicondylitis relates to the common flexor origin. The pronator teres and flexor carpi radialis tendons insert on the anterior aspect of the medial epicondyle and are the most commonly affected. This is commonly known as golfers’ elbow or medial epicondylitis. It can also occur in other daily activities with repeated wrist flexion and protonation such as bowling, pitching, carpentry, and in the playing of stringed instruments. Radiographs may show traction spurs around the humeral medial epicondyle. It is best identified by MR imaging. The tendons do not commonly tear and if they do this usually occurs in combination with medial collateral ligament injury. Tendinosis will have similar appearances to common extensor origin tendinosis on MR imaging. Pronator teres muscle tears rarely occur when a bat or club hits the ground during a vigorous swing during cricket or golf, and flexor carpi ulnaris and digitorum superficialis muscle tears were observed at the London Olympic Games 2012
The ulnar collateral ligament (UCL) of the elbow can be injured in throwing athletes. This will be a cause of medial-sided elbow pain. It can be injured at the same time as the medial tendons. In the United Kingdom, this is most commonly seen in javelin throwers, but in the United States, baseball pitchers are more frequently affected. If there is a complete tear, a radiograph can demonstrate widening of the medial joint line. Any associated avulsion fractures with this injury will often be identified on a radiograph. Calcification may also be seen within an injured UCL on a radiograph. The ligament will become thickened and edematous and will be seen on a fluid-sensitive MR sequence as high signal intensity. The ligament can sometimes remain intact despite an avulsion fracture of the sublime tubercle of the coronoid process of the ulna and will be seen as a detached fragment of bone. For this, T1 spin echo sequences are useful.
The ulnar nerve is in close proximity to these other structures and can be injured concomitantly or be a cause of pain in itself. Ulnar nerve abnormalities will be discussed in more detail in the section on neurologic symptoms.
Snapping triceps syndrome is caused by the medial head of the triceps muscle dislocating over the medial epicondyle in elbow flexion beyond 100°. It can be congenital or acquired. Congenital problems include an accessory triceps tendon or hypoplastic bone. Acquired hypertrophic musculature in weightlifters can lead to snapping. This can be a cause of pain in itself, but it can also cause ulnar neuritis. There is no specific radiographic feature that relates to this diagnosis.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


