TABLE 31.1 Classification of Shunt Lesions | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 31.2 Group V Lesions | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
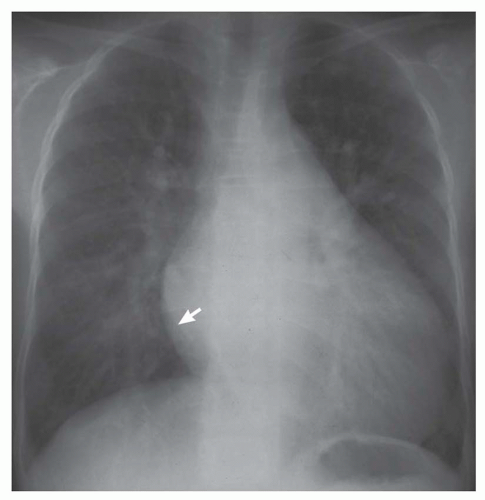 FIG. 31-1. Patent ductus arteriosus. Note pulmonary arterial overcirculation and cardiomegaly. Pulmonary arterial overcirculation is indicated by prominent hilar vessels. There is a left atrial double density (arrow) and enlarged aortic arch. |
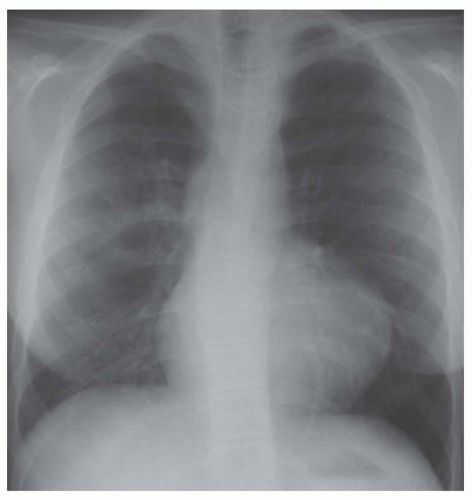 FIG. 31-2. Tetralogy of Fallot. Note decreased pulmonary vascularity without cardiomegaly. The main pulmonary arterial segment is concave and the hilar vessels are small. The apex is situated high above the diaphragm. |
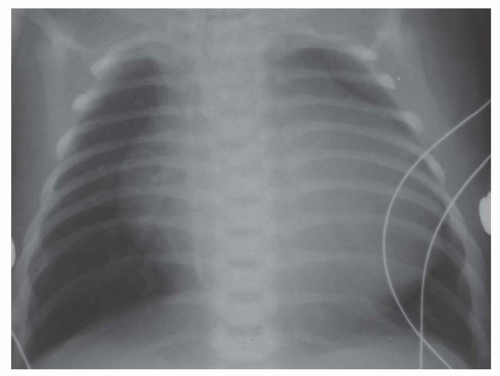 FIG. 31-3. Ebstein’s anomaly. Note decreased pulmonary vascularity with cardiomegaly. Hilar vessels are small and segmental pulmonary arteries are hardly visible, especially in the upper lobes. Vector of enlargement of the apex of the heart is directly lateral, indicating right ventricular enlargement. |
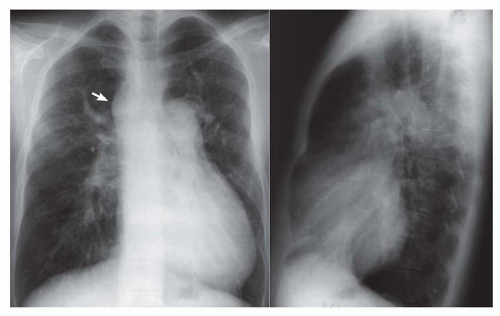 FIG. 31-4. Truncus arteriosus, type I. Note pulmonary arterial overcirculation in the presence of cyanosis and cardiomegaly. There is an enlarged aorta with right arch (arrow). |
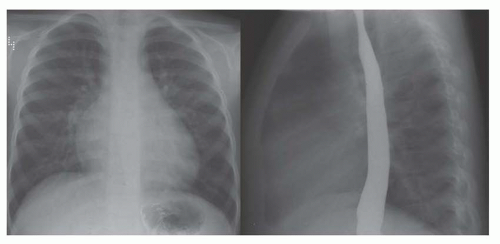 FIG. 31-5. Atrial septal defect. Frontal (left) and lateral (right) views. Pulmonary arterial overcirculation is shown by large hilar and segmental pulmonary arteries. The absence of left atrial enlargement, indicated by no impression on the barium-filled esophagus, is characteristic for an atrial-level shunt. |
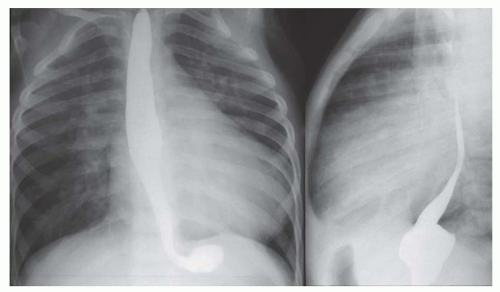 FIG. 31-6. Ventricular septal defect. Frontal (left) and lateral (right) views. Pulmonary arterial overcirculation is evidenced by shunt vessels and prominent hilar vessels. Heart size is increased in proportion to overcirculation. Left atrial enlargement produces impression on and displacement of the barium-filled esophagus, as shown on the lateral view. |
When cardiomegaly exists out of proportion to the pulmonary arterial vascularity, then one must consider a number of possibilities. One of the possibilities is that the left-to-right shunt is diminishing in size because of a decrease in the size of the ventricular septal defect (VSD). Another consideration is the coexistence of additional cardiac lesions, such as primary myocardial disease or coarctation of the aorta.
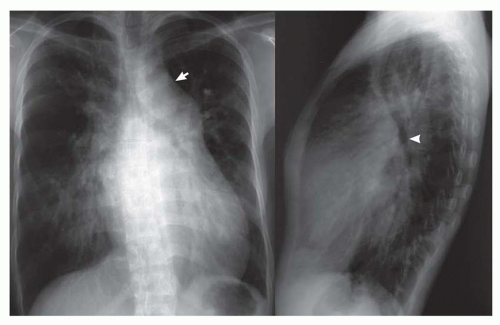 FIG. 31-7. Patent ductus arteriosus. Frontal (left) and lateral (right) views. Note pulmonary arterial overcirculation and cardiomegaly. The prominent aortic arch (arrow) and descending aorta are diagnostic signs of patent ductus arteriosus. On the lateral view, the enlarged left atrium causes posterior displacement of the left bronchus (arrowhead). |
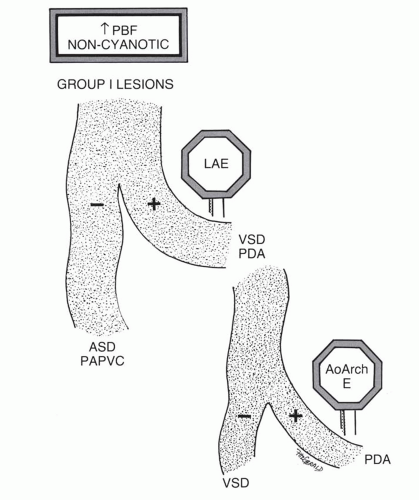 FIG. 31-8. Signposts on the diagnostic pathway of left-to-right shunts. |
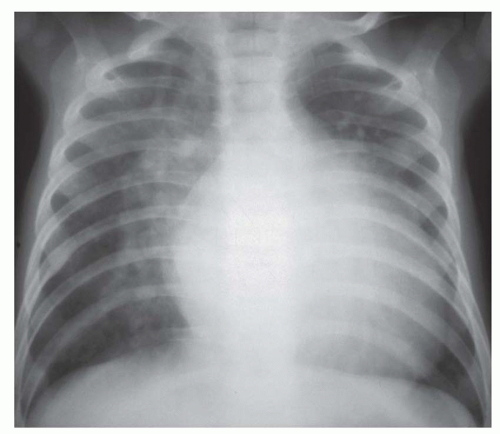 FIG. 31-9. Ventricular septal defects. Large-volume left-to-right shunt causing pulmonary edema, severe pulmonary arterial overcirculation, and cardiomegaly. Indistinct hilar and segmental arteries on the right side are caused by interstitial edema. |
involves a nonrestrictive intracardiac shunt and a severe obstruction to pulmonary blood flow. The nonrestrictive intracardiac shunt permits equalization of the pressures between two chambers, and this prevents substantial enlargement of the right ventricle. Consequently, there is usually little or no cardiomegaly. An example of the importance of the size of the intracardiac defect is in patients with tricuspid atresia. The patient with tricuspid atresia with a large atrial septal defect demonstrates little or no cardiomegaly (Fig. 31-12). On the other hand, the patient with tricuspid atresia with a restrictive atrial septal defect experiences substantial right atrial enlargement, which results in cardiomegaly. Consequently, the former patient would be classified in group II, the latter patient in group III. Tricuspid atresia can be classified in group IV when there is an associated increase in pulmonary blood flow, which is caused by either a large left-to-right shunt at the ventricular septal level or the concurrence of transposition of the great vessels. Transposition of the great arteries (TGA) occurs in approximately 30% of patients with tricuspid atresia.
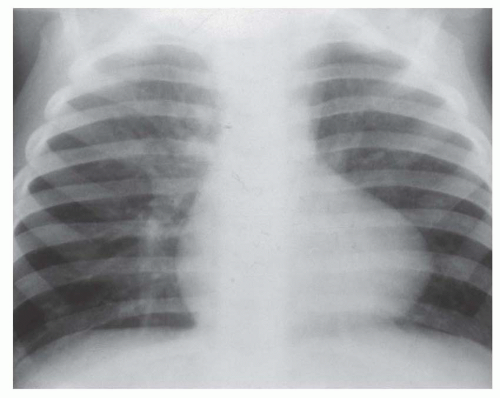 FIG. 31-10. Tetralogy of Fallot. Note pulmonary oligemia with more diminished vascularity on the left, especially the left upper lobe. Normal heart size and concave pulmonary artery segment are characteristic features in the infant. |
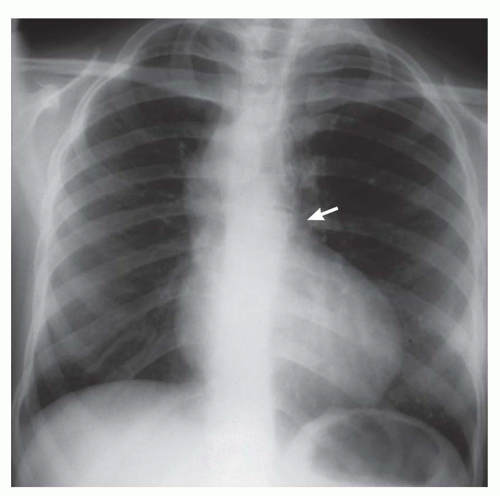 FIG. 31-11. Pulmonary atresia with ventricular septal defect (severe tetralogy of Fallot). Pulmonary oligemia, absent main pulmonary artery segment (arrow), and normal heart size are characteristic features. There is a right aortic arch. |
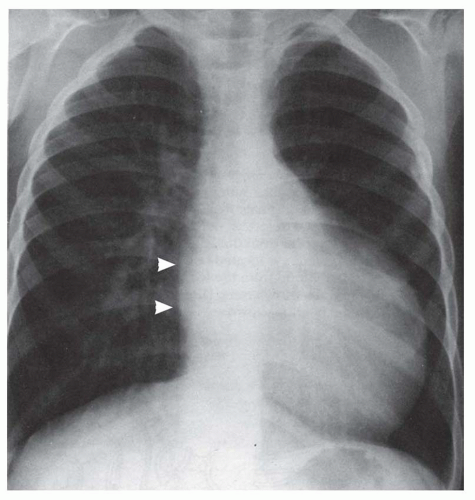 FIG. 31-12. Tricuspid atresia with large (nonrestrictive) atrial septal defect. There is decreased pulmonary vascularity and only mild cardiomegaly. Note the flattened right atrial border (arrows), which is characteristic for this lesion when there is a large nonrestrictive atrial septal defect. |
prompt the diagnostic consideration of a lesion causing tricuspid regurgitation.
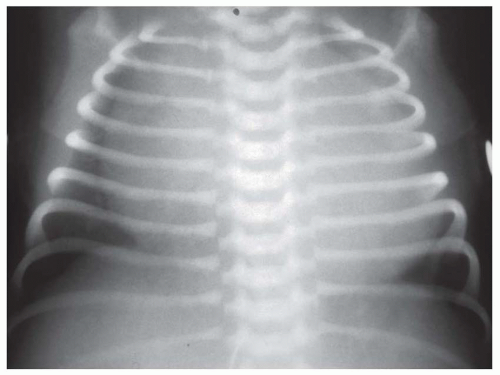 FIG. 31-13. Pulmonary atresia with intact ventricular septum, type II. Substantial tricuspid regurgitation in association with this anomaly (type II) causes right-sided chamber enlargement, especially right atrial enlargement. |
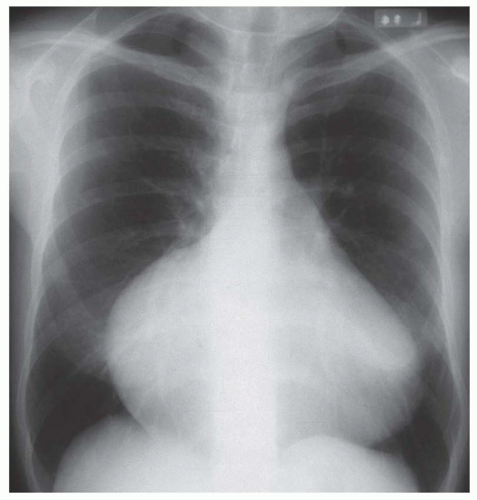 FIG. 31-14. Ebstein’s anomaly in an adult. Note decreased pulmonary vascularity and marked cardiomegaly. The prominent bulging and elongation of the right heart border are indicative of severe right atrial enlargement. |
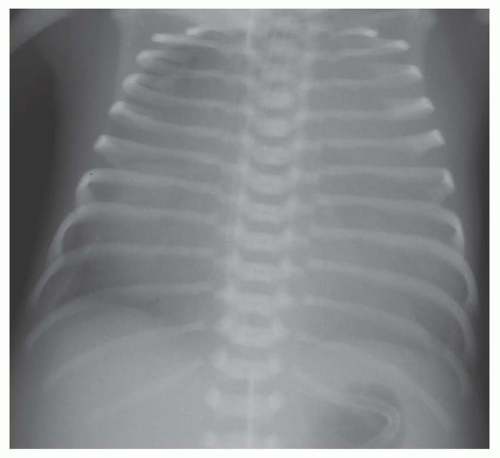 FIG. 31-15. Tricuspid regurgitation of the newborn. Pulmonary vascularity is decreased and marked cardiomegaly is present due to right-sided chamber enlargement. Extreme cardiomegaly producing the “wall-to-wall” heart is usually due to severe tricuspid regurgitation. |
total anomalous pulmonary venous connection (Fig. 31-18), tricuspid atresia, and single (“tingle”) ventricle. Doubleoutlet right ventricle and double-outlet left ventricle are also considered in this category, but these can be brought to mind when one thinks of TGA, since these lesions are essentially hybrids of TGA. The lesion that is frequently forgotten in this group is multiple pulmonary arterial venous malformations. The patient with multiple pulmonary arterial venous malformations is frequently mildly or even moderately cyanotic, and because of the several malformations within the lung, there is the appearance of increased pulmonary arterial vascularity.
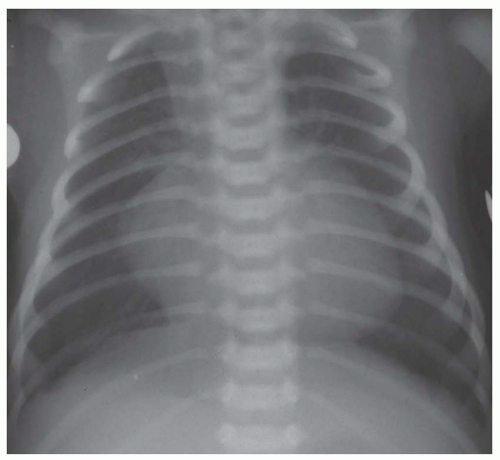 FIG. 31-16. Transposition of the great arteries. Pulmonary arterial overcirculation and an ovoid heart with a narrow base (vascular pedicle) of the heart are characteristic features. |
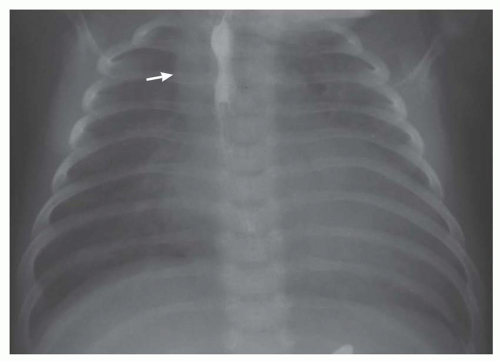 FIG. 31-17. Truncus arteriosus. Pulmonary arterial overcirculation and right aortic arch (arrow) are characteristics of truncus arteriosus. |
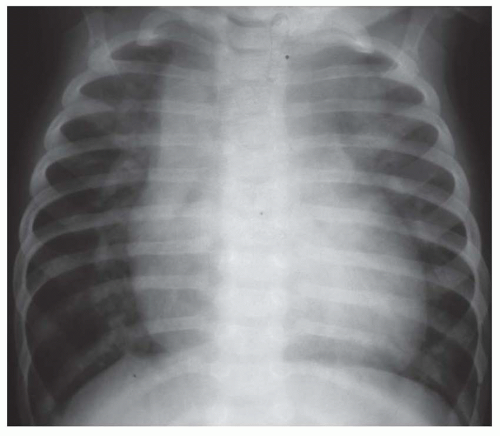 FIG. 31-18. Total anomalous pulmonary venous connection, supracardiac type (type I). Note pulmonary arterial overcirculation and cardiomegaly. Enlargement of supracardiac region is caused by an enlarged left-sided vertical vein and a dilated right superior vena cava; it is characteristic of this anomaly. |
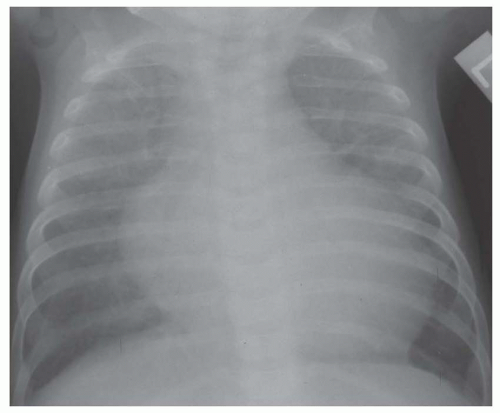 FIG. 31-19. Endocardial fibroelastosis. Pulmonary edema and cardiomegaly are characteristic features of group V lesions. |
usually consist of dyspnea, tachypnea, and tachycardia. The salient radiographic findings are indistinctness of the pulmonary vascularity, especially in the perihilar area, or interstitial pulmonary edema (see Figs. 31-19 and 31-21). Another observation that places a lesion into this group is disproportionately prominent cardiomegaly in comparison to the prominence of pulmonary vascularity (see Figs. 31-19 and 31-20).
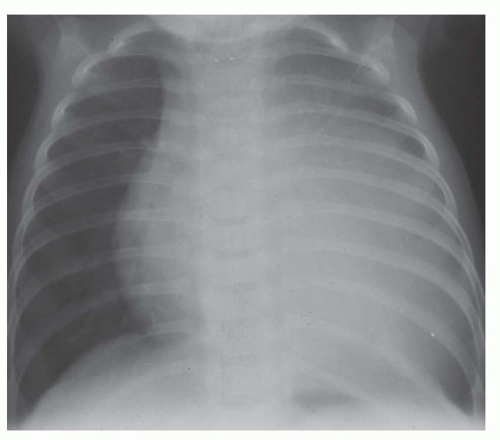 FIG. 31-20. Anomalous origin of the left coronary artery from the pulmonary artery. Cardiomegaly is disproportionate to pulmonary vascularity in a noncyanotic infant. Left atrial enlargement (right retrocardiac double density) is caused by mitral regurgitation from papillary muscle infarction. |
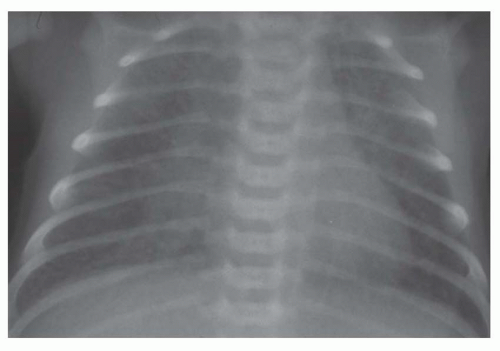 FIG. 31-21. Total anomalous pulmonary venous connection, type III. Radiograph shows pulmonary edema and normal heart size. |
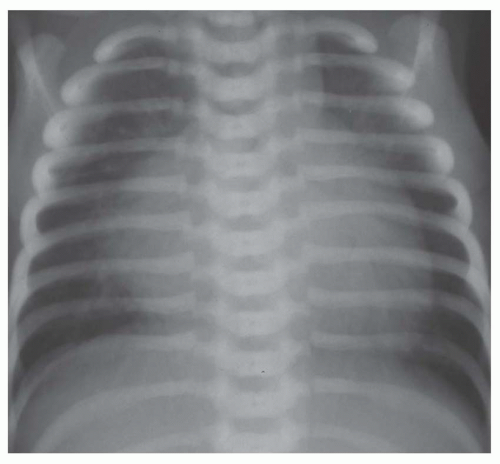 FIG. 31-22. Hypoplastic left heart. Note pulmonary venous congestion and edema and cardiomegaly. Prominent right atrium and ventricle and posterior aortic arch are characteristic features of this lesion. |
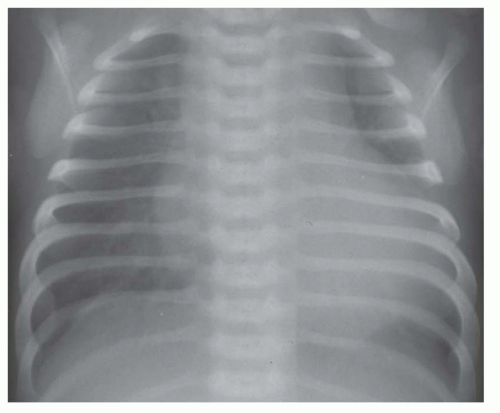 FIG. 31-23. Severe coarctation of the aorta in a newborn. There is marked cardiomegaly with pulmonary edema. |
vena cava or in the lower septum and bordering on the ostium of the inferior vena cava. A rare type of defect occurs at a site normally occupied by the coronary site and coexists with absence of the wall separating the coronary sinus from the left atrium so that the associated left superior vena cava enters into the left atrium. The coexistence of large primum and secundum defects constitutes a common atrium.
TABLE 31.3 Salient Radiographic Features of Atrial Septal Defect | ||||||
|---|---|---|---|---|---|---|
|
TABLE 31.4 Salient Radiographic Features of Atrial Septal Defect with Pulmonary Arterial Hypertension | |||||
|---|---|---|---|---|---|
|
TABLE 31.5 Salient Radiographic Features of Partial Anomalous Pulmonary Venous Coarctation | ||||||||
|---|---|---|---|---|---|---|---|---|
|
even in patients with substantial mitral regurgitation (Table 31-7; Figs. 31-27 and 31-28).
TABLE 31.6 Salient Radiographic Features of Scimitar Syndrome | |||
|---|---|---|---|
|
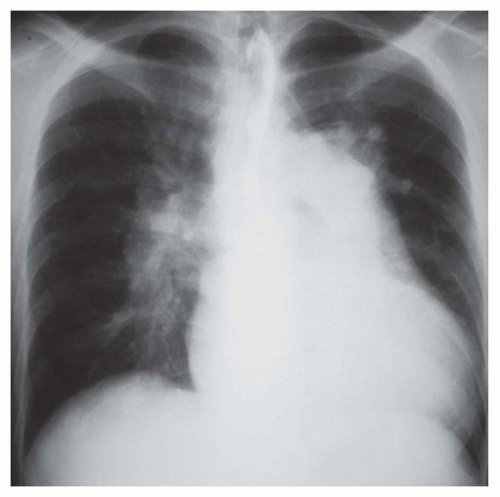 FIG. 31-24. Atrial septal defect in an adult. The radiograph shows pulmonary arterial overcirculation and cardiomegaly due to right-sided chamber enlargement. Severe dilatation of the central pulmonary arteries is a feature of this anomaly in the adult. The right pulmonary artery is very prominent. |
by malposition of the outlet septum, resulting in a small right ventricular outflow region and an aorta overriding the septal defect (tetralogy of Fallot). VSDs are not uncommonly multiple. Multiple defects in the trabecular septum may produce a “Swiss cheese septum.”
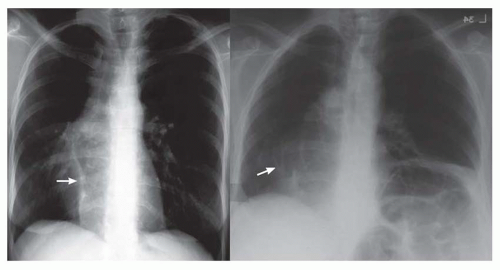 FIG. 31-25. Two patients with scimitar syndrome. Left: Radiograph showing a scimitar vein near the right diaphragm, a dextroposed heart, and a small right lung. The scimitar vein (arrow) enlarges in its course toward the diaphragm. Right: Radiograph showing multiple anomalous veins (arrow) arching toward the right hemidiaphragm. The increased diameter of the veins from superior to inferior indicates that they are anomalous veins rather than pulmonary arteries. The heart is dextroposed. There is an incidental eventration of the left hemidiaphragm. |
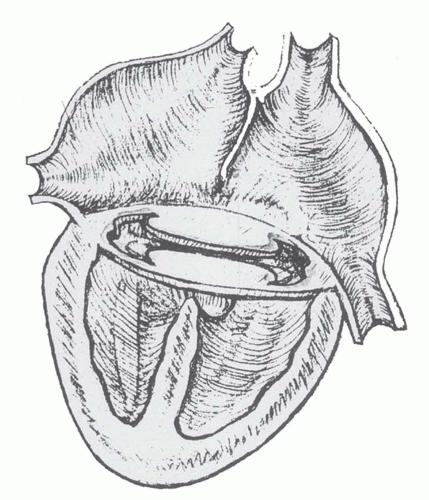 FIG. 31-26. Diagram of complete form of atrioventricular septal defect. The defect consists of a primum atrial septal defect, an inlet ventricular septal defect, and a single atrioventricular valve spanning the ventricular septal defect. |
TABLE 31.7 Salient Radiographic Features of Atrioventricular Septal Defect | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


