Extracolonic tumor extension: Irregular external (serosal) margin of rectum
Strands of soft tissue extending from serosal surface into perirectal fat
Loss of tissue fat planes between rectum and surrounding muscles and organs
Metastasis to lymph nodes at external iliac and paraaortic chain, inguinal, retroperitoneum, or porta hepatis
• Mass; pericolonic infiltration, lymphadenopathy may be shown better on MR than CT
• Transrectal ultrasonography: Best for local invasion, pelvic nodes
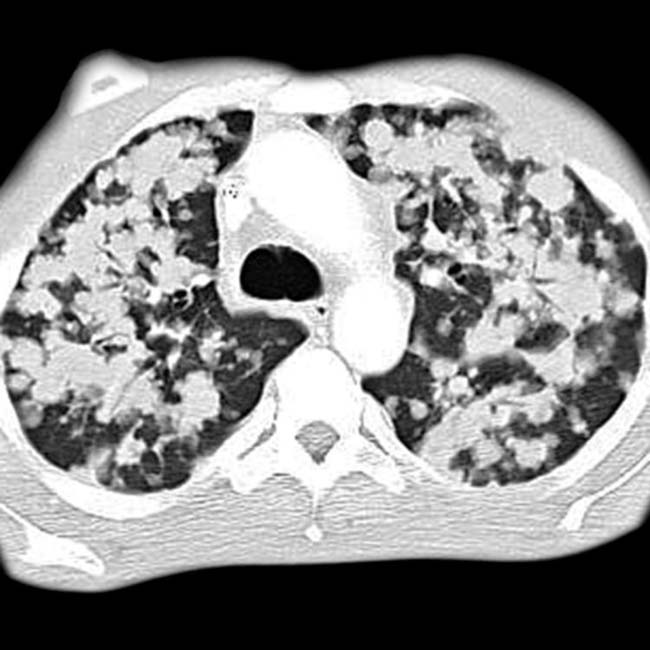
• May have lung and bone metastases before liver metastases (unlike typical pattern for colon carcinoma)
Due to dual venous drainage, including internal iliac and hemorrhoidal veins
• PET/CT: Excellent for staging and recurrence
TOP DIFFERENTIAL DIAGNOSES
• Invasion by adjacent tumor (cervix, prostate, bladder)
• Rectal villous adenoma
• Trauma or infection
PATHOLOGY
• Adenocarcinoma: Arises from mucin-producing glands (80% of rectal tumors)
• Squamous cell (cloacogenic) carcinoma (20% of rectal tumors)
DIAGNOSTIC CHECKLIST
• Image detection of perirectal tumor spread is vital; requires preoperative radiation ± chemotherapy
(Left) Axial CECT in a 68-year-old man with frequent passage of small amounts of mucus and stool shows a large rectal mass that breaks through the rectal wall , interrupting the otherwise complete rectal mucosal enhancement. There was no colonic obstruction, suggesting the soft nature of this villous carcinoma.
(Right) CT in the same patient shows extensive infiltration of the perirectal fat planes , strongly suggesting transmural spread of tumor and the need for neoadjuvant therapy prior to resection.
(Left) Transrectal ultrasonography shows a bulky rectal mass with invasion through the submucosa in this patient with T3 stage rectal carcinoma.
(Right) Axial CECT shows extensive pulmonary metastases from rectal carcinoma in a patient with no liver metastases. The dual venous drainage of the rectum (systemic and portal) explains this pattern and results in very different clinical behavior of rectal and colon cancers.
TERMINOLOGY
Definitions
• Malignant transformation of rectal mucosa
IMAGING
General Features
• Best diagnostic clue
Polypoid rectal mass with irregular surface
• Morphology
Early cancer: Sessile or pedunculated tumors
Advanced cancer: Annular, semiannular, polypoid or “carpet” tumors
Most common in rectum: Sessile and polypoid
• Other general features
Radiologic and histologic features are similar to colon carcinoma
Radiographic Findings
• Fluoroscopic-guided barium enema
Early cancer: Sessile (plaque-like) lesion
– Most typical early colorectal cancer
– Flat, protruding lesion with broad base and little elevation of mucosa (profile view)
– Discrete borders and shallow central ulcers (profile view)
– Curvilinear or undulating lines (en face view)
Early cancer: Pedunculated lesion
– Short and thick polyp stalk
– Irregular or lobulated head of polyp
Advanced cancer: Polypoid lesion
– Dependent wall: Filling defect in barium pool
– Nondependent wall: Etched in white
Advanced cancer: Semiannular (“saddle”) lesion
– Transition to annular carcinoma (“apple core”)
– Convex barium-etched margins (profile view)
Advanced cancer: Annular (“apple core”) lesion
– Circumferential narrowing of bowel; shelf-like, overhanging borders (mucosal destruction)
– High-grade obstruction and ischemia: “Thumbprinting” of dilated proximal colon
Advanced cancer: “Carpet” lesion
– Malignant villous tumor may appear as “carpet” lesion with minimal protrusion into lumen
– Radiolucent nodules surrounded by barium-filled grooves; finely nodular or reticular pattern
CT Findings
• Mass and focal or circumferential wall thickening


 Metastasis to lymph nodes at external iliac and paraaortic chain, inguinal, retroperitoneum, or porta hepatis
Metastasis to lymph nodes at external iliac and paraaortic chain, inguinal, retroperitoneum, or porta hepatis

 that breaks through the rectal wall
that breaks through the rectal wall  , interrupting the otherwise complete rectal mucosal enhancement. There was no colonic obstruction, suggesting the soft nature of this villous carcinoma.
, interrupting the otherwise complete rectal mucosal enhancement. There was no colonic obstruction, suggesting the soft nature of this villous carcinoma.
 , strongly suggesting transmural spread of tumor and the need for neoadjuvant therapy prior to resection.
, strongly suggesting transmural spread of tumor and the need for neoadjuvant therapy prior to resection.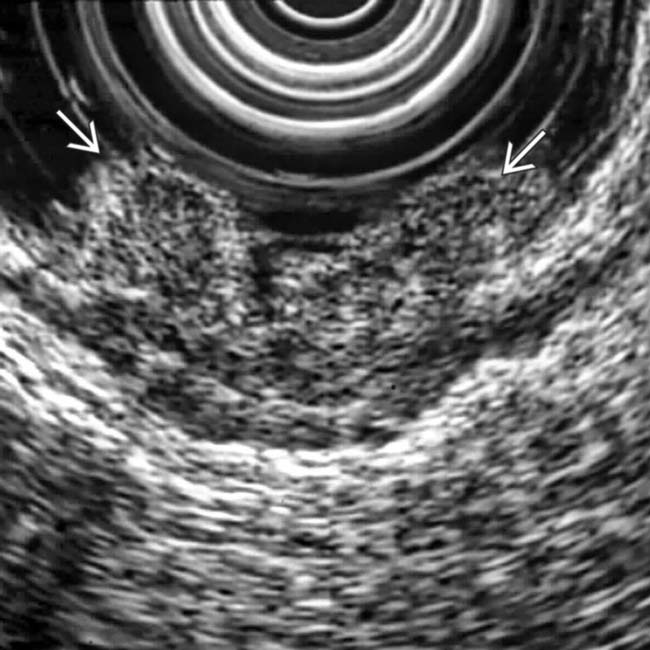
 with invasion through the submucosa in this patient with T3 stage rectal carcinoma.
with invasion through the submucosa in this patient with T3 stage rectal carcinoma.