• The right kidney is normally situated lower than the left kidney.
• The right kidney is posteroinferior to the liver and gallbladder.
• The left kidney is inferior and medial to the spleen.
• Located immediately superior, anterior, and medial to each kidney is an adrenal gland.
Anatomy
• The kidneys are described as having a superior and inferior pole, medial and lateral margins, and an anterior and posterior surface.
• The kidneys are encapsulated by a fibrous renal or true capsule.”
• Fat surrounds the encapsulated kidneys in the perinephric or perirenal space (part of the retroperitoneal space within the renal fascia that contains the kidney, perirenal fat, adrenal gland, and proximal ureter).
• Gerota’s fascia is a fibrous sheath that encloses each kidney, perinephric fat, and adrenal gland.
• Normal adult kidneys measure 9 to 12|cm long, 2.5 to 3.5|cm thick, and 4 to 5|cm wide.
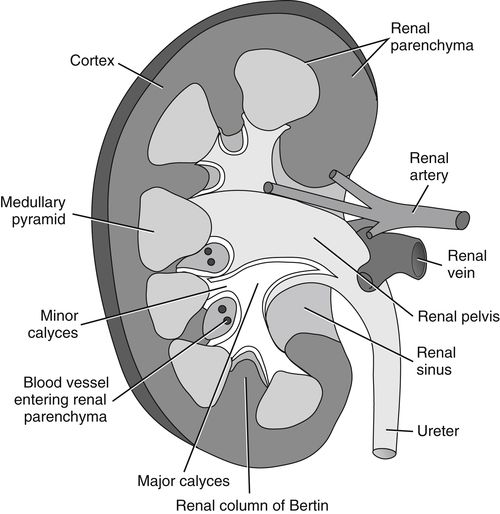
• Each kidney is composed of two distinct areas, the renal sinus and renal parenchyma:
I. Renal sinus: consists of the renal hilum and collecting system:
A. Renal hilum:
1. Medial opening into the renal sinus at the mid portion of the kidney.
2. Through it passes the renal arteries, veins, nerves, lymphatic vessels, and ureter.
B. Collecting system: consists of the infundibulum and renal pelvis:
1. The infundibulum is composed of minor and major calyces:
a. 8 to 18 minor calyces, which receive urine from the medullary pyramids (Figure 9-1).
b. 2 or 3 major calyces, which receive urine from the minor calyces then dump it into the renal pelvis.
2. The renal pelvis is a urine reservoir formed by the expanded superior end of the ureter. It receives urine from the major calyces before it is transported down the ureter to the urinary bladder.
II. Renal parenchyma: consists of the inner medulla and outer cortex:
A. Inner medulla:
1. 8 to 18 medullary pyramids that pass urine to the minor calyces in the renal pelvis. The bases of the pyramids form a margin with the renal cortex. The apices of the pyramids project into the bottom or side of the renal sinus and into the minor calyces. The pyramids are separated from each other by bands of cortical tissue referred to as the columns of Bertin, which extend inward to the renal sinus (Figure 9-2).
B. Outer cortex: The outer renal cortex lies between the medulla and outer renal capsule. It contains millions of nephrons; the microscopic functional units of the kidney that form urine.
Physiology
• As part of the excretory system, kidneys function to get rid of metabolic wastes.
• Kidneys purify the blood by excreting urine (excess water, salt, toxins).
Sonographic Appearance
• As seen in the following transverse scanning plane image of an axial section of the midportion of the right kidney, the overall sonographic appearance of the normal adult kidney is described as heterogeneous (mixed echo pattern) due to the contrast in appearance of the renal cortex and renal sinus. The renal cortex appears midgray and homogeneous (uniform echo pattern) with a smooth contour, whereas the renal sinus presents as bright with irregular borders and, in this case, interrupted with anechoic, urine-filled medullary pyramids and blood-filled vessel.

As this image demonstrates, the kidneys are easily identified by the highly reflective appearance of the surrounding renal capsule. It appears as a bright, thin continuous line seen along the periphery of the kidney, adjacent to the renal cortex. This image also shows why the kidney (cortex) is described as hypoechoic (less echogenic) compared to the adjacent normal liver.
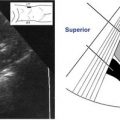
• Since the orientation of each kidney is vertically obliqued in the body; therefore, longitudinal and long axis views are seen in oblique sagittal scanning planes and oblique coronal scanning planes as demonstrated in the image on the facing page, which was taken in a coronal oblique scanning plane; it shows the long axis of a normal left kidney. Notice how the longitudinal section of the kidney appears elliptical in shape. Observe how the bases of the anechoic, urine-filled medullary pyramids form a margin with the renal cortex. In some cases, the arcuate vessels can be visualized at this corticomedullary junction as bright, echogenic dots. Note how the renal sinus appears highly reflective with variable contour due to the fat it contains.

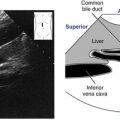
• The image below shows an axial section of the mid portion of the right kidney taken in a transverse scanning plane. The renal cortex appears homogeneous, with midgray echoes that are hypoechoic relative to the normal liver. Observe how axial sections of the kidney appear rounded and broken medially by the renal hilum. In this case, we can observe an anechoic, long section of the right renal vein exiting the renal hilum on its course to the inferior vena cava (IVC). Note the anechoic medullary pyramid. The pyramids appear anechoic or hypoechoic relative to the renal cortex depending on the amount of urine they contain. The pyramids as well as the infundibulum and renal pelvis are only visualized when they contain urine. The ureters are not normally visualized. This image also demonstrates Morison’s pouch, a peritoneal space that appears as a bright curvilinear line between the right kidney and the liver. This space is important as it is a potential site for abnormal collection of fluid.

Normal Variants
• Dromedary humps:
• Cortical bulge(s) on the lateral border of the kidney that appear the same as normal renal cortex.
• Hypertrophied column of Bertin:
• Enlarged columns of renal cortex that vary in size and indent the renal sinus.
• They appear the same as normal renal cortex.
• Double collecting system:
• The renal sinus is divided by a hypertrophied column of Bertin.
• The appearance is the same as normal renal cortex and two normal renal sinuses.
• Horseshoe kidney:
• The kidneys are connected, usually at the lower poles.
• Except for their connection, the kidneys appear otherwise normal.
• Renal ectopia:
• One or both kidneys may be found outside the normal renal fossa.
• Other locations include the lower portion of the abdominal or pelvic cavities, and in rare cases they may be found in the intrathoracic area. Except for the location, the kidney(s) appears otherwise normal.
Preparation
Patient Prep
• None.
Transducer
• 3.0 MHz or 3.5 MHz.
• 5.0 for very thin patients.
Breathing Technique
• Deep, held inspiration. Deep inspiration causes the kidneys to descend, making them easier to visualize sonographically.
Patient Position
Right Kidney
• Supine.
• Left posterior oblique, left lateral decubitus, and prone as needed.
Left Kidney
• Right lateral decubitus.
• Prone as needed.
Renal Survey Steps
Right Kidney • Longitudinal Survey
Sagittal Plane • Transabdominal Anterior Approach
1. Begin scanning with the transducer perpendicular, just inferior to the most lateral edge of the right costal margin.

2. Have the patient take in a deep breath and hold it. The longitudinal section of the kidney should come into view. If the kidney is not seen here, move the transducer small degrees in medial and inferior sections with the patient holding his or her breath, until the kidney is identified.

3. When the kidney is located, very slightly twist/rotate the transducer first one way, then the other (to oblique the scanning plane according to the vertical oblique lie of the right kidney) to resolve the long axis of the right kidney.
4. Once the long axis is determined, very slightly rock the transducer superior to inferior while slowly sliding the transducer medially, scanning through the kidney until you are beyond it.
Evaluate the perirenal region as you scan through it.

5. Move the transducer back onto the kidney. Slowly rocking and sliding scan right lateral, through and beyond the kidney.
Evaluate the perirenal region as you scan through it.

Note
The longitudinal survey of the right kidney can be performed from a coronal plane, right lateral approach. This approach can be performed with the patient supine, but it is usually easier to scan with the patient in a left lateral decubitus position.
1. Begin scanning with the transducer perpendicular, midcoronal plane, just superior to the iliac crest. Have the patient take in a deep breath and hold it as you move or angle the transducer superior to inferior or scan intercostally if necessary to locate the kidney.

2. When the kidney is identified, resolve the long axis, then very slightly rock the transducer superior to inferior while sliding the transducer anteriorly (toward the patient’s front), scanning through and beyond the kidney margin.
Evaluate the perirenal region as you scan through it.
3. Move the transducer back onto the kidney. Slowly rocking and sliding move posteriorly (toward the patient’s back), scanning through and beyond the right kidney.
Evaluate the perirenal region as you scan through it.
Right Kidney • Axial Survey
Transverse Plane • Transabdominal Anterior Approach
1. Still in the sagittal scanning plane, relocate the long axis of the right kidney. Slowly rotate the transducer 90 degrees into the transverse plane. The rounded, axial section of the kidney will come into view.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


