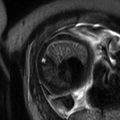
Fig. 25.1
Hemoperitoneum. (a) Axial T1-weighted gradient recalled echo image with fat saturation, (b) sagittal T2-weighted single shot turbo spin echo, and (c) axial T2-weighted turbo spin echo with fat saturation images through the pelvis demonstrate T1- and T2-hyperintense free fluid in the pelvis representing moderate-volume hemoperitoneum in a 33-year-old woman who presented with positive urine pregnancy test and acute pelvic pain due to a ruptured ectopic pregnancy. Note the large blood clot in the rectovaginal cul-de-sac (arrows)
Fig. 25.2
(a) Axial T1-weighted gradient recalled echo image and (b) coronal T2-weighted single-shot turbo spin-echo image demonstrate pneumoperitoneum in a patient following abdominal surgery. Note the air outlining the falciform ligament on the axial image (arrow)
Fig. 25.3
Solid organ injuries on CT and MR. Liver laceration and pancreatic transection in a teenage female following blunt abdominal trauma. (a, b) Axial contrast-enhanced CT images demonstrate a complex liver laceration and transection through the pancreatic neck. Selected images from an MR examination performed 2 days later demonstrate the appearance of the same injuries on (c, d) axial T1-weighted images with and without fat saturation, respectively, and (e, f) axial T2-weighted images with fat saturation. The liver laceration is seen as an irregular linear T2-hyperintense and T1-hypointense defect in the left hemiliver (arrow). There is complete disruption of the pancreatic neck with T1-hypointense and T2-hyperintense fluid within the defect (arrow)
Fig. 25.4
Diaphragmatic injury in a 24-year-old pregnant patient in a motor vehicle collision. (a) Initial chest radiograph and (b) follow-up chest radiograph obtained 4 days show development of a right hemidiaphragmatic contour abnormality, which raised concern for diaphragmatic injury. (c) Coronal and (d) sagittal T2-weighted images from a subsequent MR examination confirm herniation of the right hemiliver through a defect in the right hemidiaphragm (arrows). This was occult on the initial trauma CT examination
The primary goal in the management of pregnant trauma patients is to stabilize the mother, bearing in mind that maternal demise almost always leads to fetal demise [5]. Imaging examinations play an important role in this process as they allow for both the diagnosis and exclusion of suspected injuries. In the acute setting, injuries need to be diagnosed promptly, as maternal shock portends a poor prognosis with fetal loss rates approaching 80 % [6]. When exams are positive, they are pivotal in determining whether operative management is required and can guide surgical technique to ensure that all injuries are addressed as efficiently as possible. Negative examinations are also valuable, as they can help avoid an unnecessary laparotomy, which is beneficial given the incidence of preterm labor after nonobstetrical laparotomy is 26 % in the second trimester and 82 % in the third trimester [6, 7].
Given the need for rapid assessment of pregnant trauma patients, the workhorse imaging modalities used in this setting are conventional radiography and computed tomography (CT). These examinations can be performed rapidly and either in or very near the trauma bay, making them excellent first-line choices for the evaluation of pregnant trauma patients. There is often some initial hesitation to the use of ionizing radiation in the pregnant patient, but it is important to recognize that the risks are often poorly understood and, in the setting of a trauma, the benefits outweigh the risks. While a detailed description of the effects of radiation on the fetus is beyond the scope of this chapter and has been described elsewhere, a key point is that virtually all diagnostic imaging studies utilizing ionizing radiation that would be used in the evaluation of a pregnant trauma patient result in a fetal radiation dose of less than 50 mGy. This is important to recognize, as there are no known risks of pregnancy loss or fetal anomalies below this 50 mGy threshold [5].
25.2 Role of MRI in Imaging Pregnant Patients Involved in Trauma
There is currently no literature to support the use of magnetic resonance imaging (MRI) in the initial evaluation of a critically injured trauma patient. There are a number of factors that preclude MRI from being a viable modality in the initial evaluation of a trauma patient. MRI scanners are often physically removed from the emergency department. Transport to and from the scanners consequently uses valuable time and removes the patient from the resuscitation area. Examination times are also on the order of at least 10–15 min, which adds an additional delay. From a practical standpoint, appropriate MRI screening may be difficult if not impossible for a trauma patient with altered mental status, and family may not be readily available to provide such information.
There are certain situations, however, where MRI may be of benefit in the evaluation of a pregnant trauma patient. The primary application is in the setting of suspected spine trauma. The ACR appropriateness criteria for suspected spine trauma (2012) recommend MRI for evaluating suspected spinal cord injury, cord compression, and ligamentous injury. In these cases, MRI is complementary to, but does not replace, the initial CT of the spine [8]. MRI can also be used in the evaluation of complex musculoskeletal injuries, typically after management of life-threatening injuries has been performed.
Another potential situation for the use of MRI in the pregnant trauma patient relates to repeat or delayed abdominal imaging. For example, MRI could be used for follow-up of injuries initially seen on CT that were managed conservatively in patients who had a negative initial exam but subsequently develop symptoms or in patients who were not thought to require imaging at initial presentation but who later develop symptoms. To this end, there have been few studies evaluating the use of MRI in the nonpregnant adult population with abdominal trauma. McGehee et al. compared noncontrast MRI and contrast-enhanced CT in a small group of seven patients and concluded that MRI offered no significant advantage over CT for the evaluation of acute abdominal trauma [9]. Case reports have been published regarding the use of MRI in splenic, renal, and pancreatic injuries [10–12]. Dedicated magnetic resonance pancreatography (MRCP) protocol examinations may be useful in the evaluation of pancreatic duct injuries from blunt trauma [13]. Finally, MRI has been utilized to confirm or exclude diaphragmatic injury in patients with blunt trauma and suspicion for diaphragmatic injury [14].
25.3 Safety of MRI in Pregnancy
In the most recent American College of Radiology white paper for safe MR practices (2013), the use of MRI was deemed acceptable at any stage of pregnancy if the risk-benefit ratio to the patient warrants that the study be performed and if the required information cannot be obtained with another modality that does not use ionizing radiation [15]. Although there is no evidence of harmful effects to the fetus as a result of MRI, the main concerns are the potential effects of energy deposition and resultant tissue heating in the fetus as well as the potential effects of acoustic noise [16–18]. To minimize these potential risks, MRI of pregnant patients should be performed at field strengths of 1.5 T or less. MRI protocols should be tailored to include the minimum number of sequences required to answer the particular clinical question. In regard to the use of intravenous contrast, gadolinium is considered a pregnancy category C drug by the FDA, indicating that animal studies have shown adverse effects but adequate data are not available in humans, and the potential benefits may warrant its use in pregnant women if it is considered critical for evaluation. Typically, gadolinium-based contrast agents are not required for imaging as the necessary clinical information can be obtained from nonenhanced MRI. In rare cases in which gadolinium-based contrast material is felt to be absolutely necessary for diagnosis in a pregnant trauma patient, it can be used, but consultation with the patient regarding the potential risks and benefits is advised, if possible [19].
25.4 MRI Protocol Design for Pregnant Patients in Trauma
Choosing an appropriate MRI protocol is essential when imaging the pregnant patient in trauma. For neuro and musculoskeletal applications, standard nonenhanced protocols performed on 1.5 T scanners can answer most relevant questions. When it comes to abdominal applications, given the lack of research and experience in imaging pregnant trauma patients, or even patients involved in trauma in general, there is no standard protocol which can be broadly recommended. The important considerations in the design of a protocol for imaging the pregnant trauma patient are to choose sequences that will allow for identification of potential pathology related to trauma, namely, solid and hollow viscera injuries, hemoperitoneum, free intraperitoneal fluid, and free intraperitoneal gas. In light of safety concerns, utilizing the fewest sequences possible is recommended.
Related posts:
 Fetal MRI: Contribution to Perinatal Management and Fetal Surgical Treatment of Congenital Anomalies
Fetal MRI: Contribution to Perinatal Management and Fetal Surgical Treatment of Congenital Anomalies
 Current Techniques and Future Directions for Fetal MRI
Current Techniques and Future Directions for Fetal MRI
 Magnetic Resonance Imaging of Acute Abdominal and Pelvic Pain in Pregnancy
Magnetic Resonance Imaging of Acute Abdominal and Pelvic Pain in Pregnancy
 MRI of the Placenta
MRI of the Placenta
 Fetal Cardiovascular Magnetic Resonance
Fetal Cardiovascular Magnetic Resonance
 MR of Fetal Abdomen and Pelvis
MR of Fetal Abdomen and Pelvis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


