CHAPTER 6 Scalp
The scalp is the soft tissue covering of the calvarial vault. It extends from the eyebrows anteriorly to the external occipital protuberance and superior nuchal lines posteriorly to the zygomatic arches and external acoustic canals on both sides. It may also be designated the epicranium.
GROSS ANATOMY
Layers of the Scalp
Grossly, the scalp has five layers.1 From superficial to deep, these include (Figs. 6-1 to 6-3):
• The skin proper, composed of the epidermis and dermis
• The superficial fascia, consisting of firm dense adipose tissue deep to and closely adherent to the skin
• The epicranial aponeurosis, a continuous fibromuscular sheet composed of the occipitofrontalis muscle, the temporoparietalis muscles, and their associated epicranial aponeurosis (synonym: galea aponeurotica)
• The loose subgaleal areolar tissue

FIGURE 6-1 Coronal cross section of the scalp. This diagram depicts the relationships of the superficial epidermis and dermis, the prominent, radially oriented septations of the superficial fascial layer, the locations of the major blood vessels within the superficial fascial layer, and the valveless emissary veins connecting the subgaleal loose areolar tissue with the diploic space of the calvaria and with the intracranial dural venous sinuses.
(Modified from Standring S, Berkovitz BK. Face and scalp. In Stranding S, Ellis H, Healy JC, et al [eds]. Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 39th ed. Philadelphia, Elsevier, 2005, p 497.)
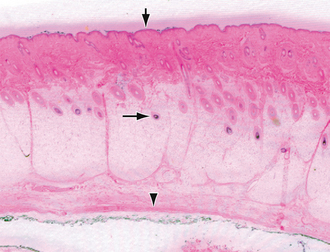
FIGURE 6-2 Hematoxylin and eosin stain of the scalp superficial to the subgaleal loose areolar connective tissue layer. The downward-pointing arrow indicates the epidermis at the skin surface. The dermis lies immediately subjacent to this and shows multiple hair follicles and related glands. The horizontal arrow indicates the bulb of the hair follicle in the subdermal adipose tissue of the scalp. The bulb is the deepest portion of the hair apparatus. The arrowhead indicates the deep surface of the galeal aponeurosis.
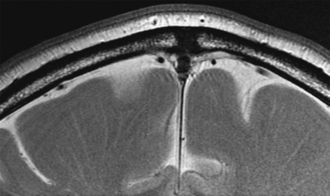
FIGURE 6-3 High-resolution T2W MR image of the scalp depicts the slightly undulating contour of the interface of the skin with the superficial fascia due to the presence of hair follicles. The subgaleal soft tissue and pericranium blend in with the signal void of the external cortical surface of the calvaria.
The scalp also contains the arteries, veins, lymphatics, and nerves that supply the soft tissue.
Skin Proper
The skin overlying the calvaria is continuous with the skin of the face and neck. It is generally thinnest anteriorly at the forehead, where it measures approximately 3 mm, and it is thickest posteriorly at the occiput, where it measures up to 8 mm. The skin is usually slightly thicker in women than men. It gradually increases in thickness from childhood until age 35 years (women) or 55 years (men) and then begins to show thinning and atrophy.2
Superficial Fascia
The superficial fascial layer varies in thickness. It measures 4 to 6 mm in people of normal weight but 20 mm or more in obese individuals. Within this layer, multiple, vertically oriented reticular fibers divide the layer into small compartments (Figs. 6-4 and 6-5). These septa form strong connections between the superficial dermis and the subjacent galea aponeurotica. As a consequence, the subcutaneous layer is relatively inelastic and the dermis, subcutaneous tissue, and galeal aponeurosis move together as one unit.
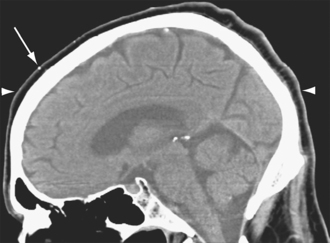
FIGURE 6-4 Sagittal reformatted noncontrast CT of the head. The skin (arrowheads) is thinner anteriorly and thicker posteriorly. A small cutaneous calcification (arrow) is noted.
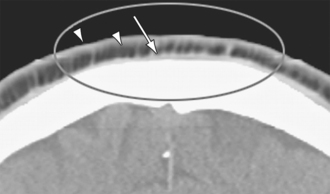
FIGURE 6-5 Coronal reformatted noncontrast CT of the head depicts the isodense skin (left arrowhead) superficially, the thick lucent adipose tissue of the superficial fascial layer (right arrowhead) in the middle, and the thick isodense deeper tissue (arrow) representing the combined galea aponeurotica, subgaleal loose areolar tissue, and pericranium. Individual septations cross and partially subdivide the adipose tissue of the superficial fascial layer.
The subcutaneous layer has a rich network of arteries, veins, and lymphatics. The arteries are tethered to the fibrous septa, so they are relatively immobile and unable to constrict quickly after a laceration.3
Subgaleal Connective Tissue
The subgaleal connective tissue is a largely avascular, filmy layer of loose fibroareolar tissue interposed between the galea aponeurotica superficially and the pericranium deeply. Anteriorly, the subgaleal layer extends deep to the frontalis and orbicularis oculi muscles. Posteriorly, it extends deep to the occipitalis muscle, as low as the superior nuchal line. Laterally, the subgaleal connective tissue is limited by the attachment of the galeal aponeurosis to the superficial temporalis fascia.
The areolar tissue in this layer is only loosely connected to the subjacent pericranium, so the subgaleal layer serves as a “gliding plane” for motion of the scalp over the calvaria. As a consequence, it is easy to establish a subgaleal plane for dissection at surgery and postmortem examination.4
Muscles of the Scalp
Occipitofrontalis
The occipitofrontalis is the major muscle complex of the epicranium. It is composed of the paired frontalis muscles anteriorly and the paired occipitalis muscles posteriorly. These muscles are interconnected by the galea aponeurotica (Fig. 6-6).5 Each frontalis muscle is a thin quadrilateral sheet of muscle that is attached to the overlying superficial fascia externally (especially at the eyebrows) and that ascends into the galea aponeurotica anterior to the coronal suture. The frontalis muscle has no bony attachment.4 The medial margins of the two frontalis muscles blend together above the nasal root. The medial fibers of each frontalis muscle continue inferiorly to become continuous with the procerus (see later). The intermediate fibers of the frontalis blend with the orbicularis oculi and the corrugator supercilii (see later). The lateral fibers of the frontalis muscles blend with the lateral portions of the orbicularis oculi over the zygomatic processes of the frontal bones.5 Because the frontalis has no bony anchor, hematomas and other pathologic processes may extend anteriorly and inferiorly, deep to the aponeurotic sheath, to reach the eyelids. Posteriorly, the paired quadrilateral shaped occipitalis muscles arise by tendinous fibers from the lateral two thirds of the superior nuchal lines of the occipital bone and mastoid processes of the temporal bones. They insert into the galea aponeurotica at a level slightly above the superior aspect of the auricles.
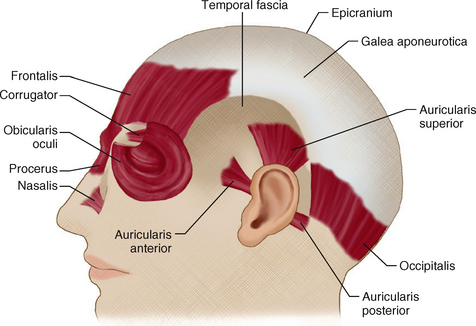
FIGURE 6-6 Muscles of the scalp. The largest scalp muscle is the epicranius, composed of paired anterior muscle bellies, named the frontalis, and paired posterior muscle bellies, named the occipitalis. Between these muscles is an aponeurotic sheath, named the galea aponeurotica. The temporalis muscle lies deep to the temporal fascia. The auricular muscles arise from this sheath to insert on the external ear.
(Modified from Lewis WH. Henry Gray’s Anatomy of the Human Body, 20th ed. Philadelphia, Lea & Febiger, 1918, p 379.)
The paired frontalis muscles work in conjunction to elevate the eyebrows and forehead and to produce the characteristic transverse creases of the forehead. The occipitalis acts in conjunction to tighten the scalp. In many individuals they do not demonstrate any motion.6 Both the frontalis and the occipitalis are innervated by the facial nerve—the frontalis by temporal branches of the facial nerve and the occipitalis by occipital branches of the facial nerve.
Procerus
The procerus is a small pyramidal slip of muscle that extends downward from the skin of the forehead between the eyebrows and from the medial portions of the frontalis muscles to join a fascial aponeurosis that covers the lower nasal bones and the adjacent lateral nasal cartilages (see Fig. 6-6).5
Orbicularis Oculi
The orbicularis oculi is a broad flat elliptical muscle that extends into the eyelids, surrounds the orbital aperture, and spreads circumferentially into the anterior temporal region, the infraorbital cheek, and the superciliary region (see Fig. 6-6).5 It has three parts:
1. The thick orbital portion of the orbicularis oculi attaches medially to the nasal process of the frontal bone, the frontal process of the maxilla, and the intervening medial palpebral ligament. Its upper portion blends with the frontalis muscle and the corrugator supercilii on each side.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


