Case presentation
A 15-month-old boy is brought into the emergency department by his parents for inconsolable crying for the last 6 hours. He has been crying and refusing to feed and has had nonbloody, nonbilious emesis twice. He is afebrile and his other vital signs are heart rate in the 160s beats per minute, respiratory rate of 30 breaths per minute, blood pressure of 107/89 mm Hg, and an oxygen saturation of 98% on room air. He is asleep and does not wake up except to grimace during his abdominal examination. There are no deformities, corneal abrasions, and other abnormalities on the rest of his examination.
Imaging considerations
Imaging modalities largely depend on institutional practices, the availability of fluoroscopy and ultrasound (US), and the experience and preference of the providers managing the patient. A prompt surgical consult is warranted in children with obvious signs of peritonitis as operative management is required. For children who are not in extremis, several imaging choices are available to clinicians.
Plain radiography
A two-view study (anterior-posterior and upright or preferably left lateral decubitus) is preferred to look for signs of obstruction (dilated bowel loops, air fluid levels) or for bowel perforation (free air), especially prior to any attempted enema reduction or surgical intervention. However, given the reported low sensitivity (48%) and specificity (21%) of plain film for intussusception in pediatric patients, abdominal radiographs in general should not to be used exclusively to exclude the diagnosis of intussusception. Left lateral decubitus views are favored over upright views in young children at greatest risk for intussusception. On upright views, gas moves superiorly, with decreased gas in the cecum and distal colon, which can cause spurious concern for intussusception. On left lateral decubitus views, colonic gas moves into the cecum and right colon, the area of greatest concern with suspected intussusception. Findings, which depend on the duration of symptoms and degree of associated complications, that suggest abnormality include:
- ▪
Other signs of obstruction: proximal bowel dilation with distal paucity of gas ( Figs. 16.1 and 16.2 ).
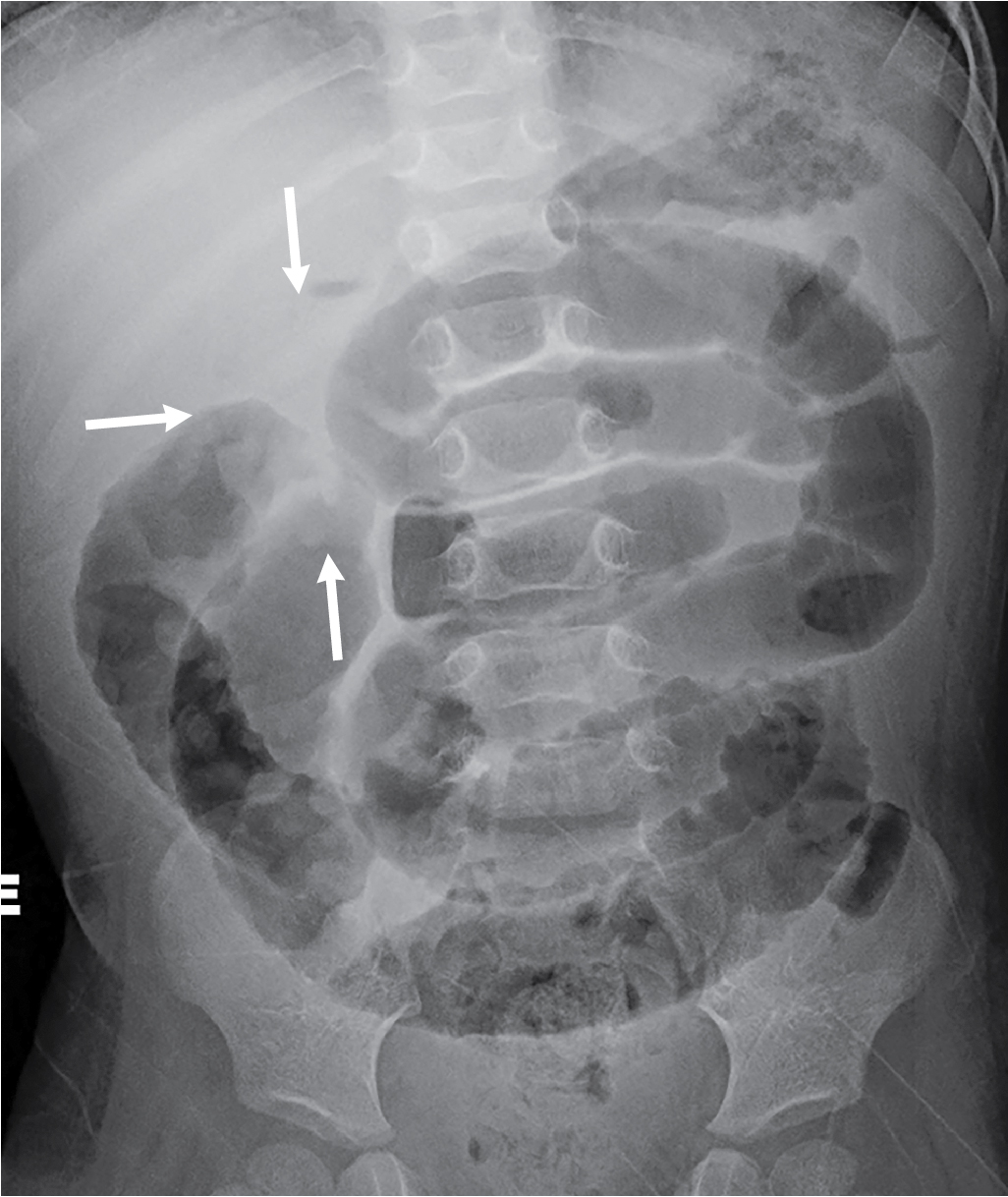
Fig. 16.1
Anterior-posterior view demonstrating abnormal bowel gas pattern with a paucity of gas in the colon. Tubular, dilated, gas-filled loops of small bowel are consistent with small bowel obstruction. There is a subtle mass effect suggesting an intussusception in the right upper quadrant (arrows) .

Fig. 16.2
Left lateral decubitus view demonstrating small bowel obstruction, scattered air fluid levels, and no free air.
- ▪
Right upper quadrant findings of an elongated or rounded mass (see Fig. 16.1 ), obscured liver margin, or a focal paucity of gas.
- ▪
Target sign superimposed over the right kidney, with central fat within a rounded area of mass effect.
- ▪
Meniscus sign: a rounded soft-tissue mass (the intussusceptum) protruding into the gas-filled transverse colon can be seen on plain radiography, but the equivalent is well seen on an included image from an air enema ( Fig. 16.3 A).

Fig. 16.3
Selected images of air enema reduction. (A) Intussusception (arrow) encountered in the mid transverse colon. (B) Residual filling defect of an intussusception (arrows) in the air-filled cecum, consistent with partial reduction. The intussusception was subsequently completely reduced.

Abdominal US
US has a 98% to 100% sensitivity and 88% to 100% specificity for diagnosing intussusception and a negative predictive value approaching 100%. This makes it the preferred method of choice for diagnosis. The lack of ionizing radiation and the rapidity of the scanning time make this modality ideal in the pediatric population. However, US for intussusception may not be readily available at nonpediatric centers as familiarity with this technique may be lacking, and experience and expertise are needed to obtain and interpret imaging. US may also be used as the guiding imaging modality during hydrostatic reduction of intussusception and to identify underlying pathology such as polyps or other lead points not readily detected by fluoroscopy. Findings on US that suggest intussusception include the following:
- ▪
Target sign (or bull’s-eye or doughnut sign) showing the different intestinal layers of concentric bowel loops, represented by alternating echogenic and hypoechogenic bands, seen on scanning transversely through an intussusception ( Fig. 16.4 ).










