SECTION IV GASTROINTESTINAL IMAGING
Essentials 1
Case
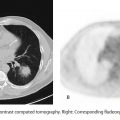
This patient is status post a single gunshot wound to the abdomen, with an entrance and exit wound on physical examination.

Questions
1. Which of the following best describes the computed tomography (CT) findings?
A. Ectopic gas has been introduced by the bullet; there is no organ injury.
B. Findings are concerning for colonic injury.
C. Gunshot wounds are sterile, regardless of bullet path.
D. No evidence of bowel injury, as there is no spillage of bowel contents.
2. What is the best next step?
A. Supportive care
B. Follow-up CT
C. Surgical evaluation
D. Barium enema
3. INDIRECT signs of penetrating bowel injury include which ONE of the following?
A. Interloop fluid
B. Bowel discontinuity
C. Leakage of oral contrast
D. Presence of an exit wound in the bowel wall
Answers and Explanations
Question 1
B. Correct! Findings are concerning for colonic injury. The path of the bullet is visible on the coronal and axial images. The proximity of the bullet path to the ascending colon must lead to a high index of suspicion for a bowel injury. The presence of pericolonic gas and fat stranding add further worry. In this patient, a through and through bowel injury was found at surgery.
Other choices and discussion
A. Ectopic gas is often introduced by bullet injuries. Indeed, the gas superficial to the anterior abdominal wall might be due to this mechanism. However, the deeper gas adjacent to the colon is not clearly due to the bullet alone, and colon injury should be suspected.
C. Gunshot injuries are not intrinsically sterile, especially when they traverse the gastrointestinal tract or the airways.
D. Spillage of bowel contents would be a direct sign of bowel injury, but the reverse is not true, and the absence of extraluminal bowel contents does not exclude injury.
Question 2
C. Correct! In the presence of penetrating trauma and bowel injury, surgical exploration is indicated.
Other choices and discussion
A. Supportive care is unlikely to result in resolution of the bowel injury without complications.
B. Follow up CT is not likely to provide any further diagnostic information at this point.
D. Barium enema is specifically contraindicated in this patient. Free barium from a leak can result in barium peritonitis, which can be difficult to treat or even life threatening. If a fluoroscopic examination is desired to confirm a bowel leak, this exam should be performed with water-soluble contrast.
Question 3
A. Correct! Direct signs of penetrating bowel injury are diagnostic of injury and include bowel wall discontinuity, wound tract extension to the bowel, leakage of oral or rectal contrast material, and active mesenteric vascular extravasation. Indirect signs may arise secondary to a bowel injury and should raise suspicion. Indirect signs of penetrating bowel injury include fat stranding, interloop fluid, and mesenteric hematoma.
Other choices and discussion
B. Bowel discontinuity is a direct sign of bowel injury.
C. Leakage of oral contrast is a direct sign of bowel injury.
D. The presence of an exit wound in the bowel wall is a direct sign of bowel injury.
Suggested Readings
Karanikas ID, Kakoulidis DD, Gouvas ZT, Hartley JE, Koundourakis SS. Barium peritonitis: a rare complication of upper gastrointestinal contrast investigation. Postgrad Med J 1997;73(859):297–298 Lozano JD, Munera F, Anderson SW, Soto JA, Menias CO, Caban KM. Penetrating wounds to the torso: evaluation with triple-contrast multidetector CT. Radiographics 2013;33(2):341–359Top Tips
Direct CT signs of bowel injury: bowel wall discontinuity, wound tract extension to the bowel, leakage of oral or rectal contrast material, and active mesenteric vascular extravasation of contrast material. These are diagnostic of bowel injury.
Indirect CT signs of bowel injury: fat stranding, mesenteric hematoma, and interloop fluid. These may arise secondary to an injury and should raise suspicion.
Always look carefully for subtle signs of bowel injury, and never assume that ectopic gas is from bullet entry alone!
Essentials 2
Case
A 39-year-old woman presents with progressive abdominal pain. Computed tomography and fluorodeoxyglucose-positron emission tomography images are shown.

Questions
1. What is the MOST likely diagnosis?
A. Adenocarcinoma
B. Linitis plastica
C. Breast cancer metastasis
D. Gastrointestinal stromal tumor
2. What is the most common location for these tumors?
A. Esophagus
B. Stomach
C. Small bowel
D. Colon
3. What is the most likely site of metastasis for these tumors?
A. Liver
B. Lung
C. Lymph nodes
D. Adjacent organs/mesenteric
Answers and Explanations
Question 1
D. Correct! This smoothly marginated, partially exophytic, gastric mass is most consistent with a gastrointestinal stromal tumor (GIST). GIST is a mesenchymal tumor that arises from the gastric wall and is often indolent and asymptomatic. Occasionally, these tumors may be ulcerated and/or hemorrhagic. GIST is most often seen in adults over age 40.
Other choices and discussion
A. Although adenocarcinoma is a common primary gastric mass, it is mucosal in origin. Larger masses are typically ulcerated and heterogeneous, growing concentrically along the gastric wall, unlike the test case.
B. Linitis plastica is a term that refers to a diffuse infiltrative process of the gastric wall, usually involving the submucosa. This is a descriptive term rather than a pathologic diagnosis and may be due to either neoplastic or inflammatory causes.
C. Breast cancer metastases might occur in the stomach. However, an isolated large homogeneous gastric mass would be very unlikely for breast cancer.
Question 2
B. Correct! Although GIST can occur anywhere along the gastrointestinal tract, the majority are found in the stomach (60 to 70%).
Other choices and discussion
A. GIST may occur in the esophagus, but this is rare. Mural masses in the esophagus are far more likely to be muscular (e.g., leiomyoma).
C. The small bowel, especially the duodenum, is the second most common location for a GIST (30% of tumors).
D. The colon is the least common location for a GIST.
Question 3
A. Correct! A small percentage of GISTs are malignant. When metastatic, disease most commonly spreads to the liver.
Other choices and discussion
B. Pulmonary metastases are rare in GIST.
C. Lymph node metastases are rare in GIST.
D. Contiguous/mesenteric spread of GIST is uncommon in primary disease, but can be seen in recurrence after resection.
Suggested Readings
Sandrasegaran K, Rajesh A, Rydberg J, Rushing DA, Akisik FM, Henley JD. Gastrointestinal stromal tumors: clinical, radiologic, and pathologic features. Am J Roentgenol 2005;184:803–811Top Tips
The most common location for a GIST is the stomach.
A GIST typically presents as a large, enhancing, solid mural mass.
These are usually benign, but when malignant, metastases most commonly occur in the liver.
Essentials 3
Case
An elderly woman presents with bloating and abdominal pain.

Questions
1. All of the following are in the differential diagnosis EXCEPT?
A. Lymphoma
B. Adenocarcinoma
C. Carcinoid
D. Metastasis
2. What is the most likely diagnosis?
A. Metastatic breast cancer
B. Adenocarcinoma
C. Inflammatory bowel disease
D. Small bowel lymphoma
3. Which ONE of the following is true regarding this disease process?
A. Obstruction is common.
B. Intussusception can occur.
C. The most common cell type is a T-cell lymphoma.
D. This most commonly occurs within the duodenum.
Answers and Explanations
Question 1
C. Correct! Small bowel carcinoid is unlikely to present as a large mass expanding the lumen of the small bowel.
Other choices and discussion
A. Small bowel lymphoma often has the appearance of the test case.
B. Adenocarcinoma is a common intrinsic small bowel mass and may rarely have the appearance of the test case.
D. Metastases may also have the appearance of the test case.
Question 2
D. Correct! This patient has one of the classic appearances of small bowel lymphoma. Lymphoma is the most common malignant tumor of the small bowel and may present with enlarged nodular folds, with diffuse mural thickening, or as an expansile and ulcerative, nonobstructing mass, as in this case. If disease is limited to the bowel and adjacent lymph nodes, it is termed primary small bowel lymphoma. Small bowel lymphoma may also be secondary.
Other choices and discussion
A. Breast cancer metastases may occur in the small bowel and might even have this appearance, but this is less common than lymphoma.
B. Adenocarcinoma of the small bowel is more likely to result in luminal obstruction than dilatation.
C. Inflammatory bowel disease would be very unlikely.
Question 3
B. Correct! Small bowel lymphoma can act as a lead point for intussusception.
Other choices and discussion
A. Obstruction is less common in small bowel lymphoma, as these tumors tend to be soft and pliable.
C. The most common cell type is B-cell lymphoma.
D. The most common location for small bowel lymphoma is the ileum.
Suggested Readings
Ghai S, Pattison J, Ghai S, O’Malley ME, Khalili K, Stephens M. Primary gastrointestinal lymphoma: spectrum of imaging findings with pathologic correlation. RadioGraphics 2007;27(5):1371–1388Top Tips
Small bowel lymphoma most commonly occurs in the ileum.
Obstruction from lymphoma is uncommon because these masses are soft and pliable tumors.
Small bowel lymphoma may be primary or secondary.
Essentials 4
Case
A 56-year-old woman presents to the emergency room.

Questions
1. What is the MOST likely diagnosis?
A. Carcinoid
B. Lymphoma
C. Desmoid tumor
D. Epiploic appendagitis
2. What telltale symptom might this patient have?
A. Intractable vomiting
B. Dry mouth
C. Flushing
D. Constipation
3. Which of the following appearances might be expected for carcinoid metastases in the liver?
A. Arterial hypoenhancement
B. Uptake of hepatocyte-specific contrast agents
C. Predominantly necrotic mass
D. Portal venous phase isoattenuation
Answers and Explanations
Question 1
A. Correct! This is most likely a carcinoid tumor. Small bowel carcinoid occurs most commonly in the ileum. This patient has masslike mural thickening in the distal small bowel. There is an associated masslike process in the mesentery with radiating bands of tissue retraction (desmoplastic reaction). With carcinoid, sometimes only the mesenteric metastases are visible on imaging. A loose rule of thirds is sometimes used: one-third occur in the small bowel, one-third have metastases, one-third are multiple, one-third have a second malignancy, and one-third have carcinoid syndrome.
Other choices and discussion
B. Lymphoma can occur in the bowel wall and the mesentery, but this appearance is less typical.
C. Desmoid tumor could explain the partially calcified retractile process in the mesentery, but involvement of the bowel wall would be atypical.
D. Epiploic appendagitis presents as an inflammatory process centered around a fat lobule along the serosal margin of the colon. There may be a visible central thrombosed vessel.
Question 2
C. Correct! This patient might have flushing. Tumors releasing 5-hydroxytryptamine (serotonin) may cause a constellation of symptoms termed the “carcinoid syndrome.” These symptoms may include flushing, diarrhea, abdominal pain, wheezing, and/or palpitations. There is high first-pass metabolism in the liver for serotonin released by bowel or mesenteric tumors, so carcinoid syndrome usually only occurs in the presence of liver metastases or in primary tumors outside of the gastrointestinal tract (especially the lung).
Other choices and discussion
A. Intractable vomiting might occur if the tumor has caused bowel obstruction. However, no bowel obstruction is present in the test case.
B. Dry mouth is classically seen with sympathetic overstimulation rather than with carcinoid syndrome.
D. Carcinoid tumor would be expected to cause diarrhea (not constipation).
Question 3
D. Correct! Portal venous phase isoattenuation. The classic enhancement pattern on computed tomography (CT) for carcinoid and other neuroendocrine metastases to the liver is arterial phase hyperenhancement, becoming somewhat isoattenuating to the liver on portal venous and delayed phases. Indeed, these tumors may be difficult to see on CT, if arterial phase imaging is not performed.
Other choices and discussion
A. Arterial hypoenhancement might be seen with treated metastases, but not in active metastatic disease.
B. Carcinoid metastases should be hypointense on the hepatobiliary phase during liver magnetic resonance imaging with hepatocyte-specific contrast. In fact, conspicuity on the hepatobiliary phase can be an excellent means of monitoring liver metastases.
C. Large amounts of necrosis would be atypical for carcinoid metastases in the liver.
Suggested Readings
Ganeshan D, Bhosale P, Yang T, Kundra V. Imaging features of carcinoid tumors of the gastrointestinal tract. Am J Roentgenol 2013;201:773–786Top Tips
The primary small bowel carcinoid may or may not be visible on CT.
Metastatic carcinoid in the mesentery is classically a masslike process with desmoplastic reaction. The mass may or may not be calcified.
Carcinoid liver metastases are typically hyperenhancing in the arterial phase.
Essentials 5
Case

Questions
1. What is the best explanation for the small bowel abnormality?
A. Inflammatory bowel disease
B. Shock bowel
C. Bowel ischemia
D. Lymphoma
2. What is the most common underlying cause of the major finding in this case?
A. Obstruction
B. Volume overload
C. Contrast reaction
D. Acute severe blood loss
3. Which of the following structures may also be hyperattenuating with this entity?
A. Spleen
B. Liver
C. Adrenal glands
D. Inferior vena cava
Answers and Explanations
Question 1
B. Correct! This is shock bowel. Shock bowel is characterized by marked submucosal edema with mucosal hyperenhancement. Shock bowel occurs from massive sudden blood loss in trauma patients and is a poor prognostic indicator. The appearance may also be seen with other causes of severe volume loss or hypotension. The proposed mechanism is mesenteric vasoconstriction with altered perfusion dynamics. Of note, the changes are reversible with resuscitation and do not always lead to bowel infarction.
Other choices and discussion
A. Active inflammatory bowel disease may result in mural edema and enhancement, but is not the best choice in this case.
C. Bowel ischemia may result in some mural edema and/or mucosal hyperemia. However, the mesenteric arteries and veins appear patent on the provided images, and there is no evidence of aortic atherosclerosis. For vascular pathology to affect the number of small bowel loops seen in this patient, a large central arterial or venous abnormality would be expected.
D. Lymphoma would not be expected to have the provided appearance.
Question 2
D. Correct! Acute severe blood loss is the most common cause of shock bowel.
Other choices and discussion
A. Obstruction would not be expected to have this appearance.
B. The ascites in this patient is caused by altered bowel permeability, not by volume overload.
C. The demonstrated findings would not be the primary result of a contrast reaction. Systemic anaphylaxis in a contrast reaction might result in hypoperfusion, but would not be the most common cause of the shock bowel appearance.
Question 3
C. Correct! Adrenal glands. In addition to the bowel findings and the slit-like inferior vena cava (IVC) seen on these images, hypovolemic shock may result in adrenal hyperenhancement, small aorta, delayed nephrograms, variable pancreatic enhancement with peripancreatic edema, and hypoenhancement of the liver and spleen.
Other choices and discussion
A. The spleen would typically be hypoenhancing in the setting of hypovolemic shock.
B. The liver would typically be hypoenhancing in the setting of hypovolemic shock.
D. The IVC is typically slit-like in hypovolemic shock (as in our patient), but not hyperattenuating.
Suggested Readings
Ames JT, Federle MP. CT hypotension complex (shock bowel) is not always due to traumatic hypovolemic shock. Am J Roentgenol 2009;192(5):W230–W235Top Tips
Shock bowel is characterized by marked submucosal edema and mucosal enhancement.
Associated findings can include hyperenhancement of the adrenal glands, flattening of the IVC and aorta, variable enhancement of the pancreas with peripancreatic edema, delayed nephrograms, and hypoenhancement of the spleen and liver.
The changes are reversible with resuscitation and do not always lead to bowel infarction.
Essentials 6
Case
A patient presents to the emergency room with worsening crampy abdominal pain.

Questions
1. What is the best diagnosis?
A. Colocolonic intussusception
B. Infectious colitis
C. Ischemia
D. Meckel’s diverticulum
2. Regarding this disease process, which ONE of the following statements is correct?
A. Often self-limited
B. Usually associated with adhesions
C. Most often caused by a benign mass
D. Most often caused by adenocarcinoma in adults
3. Which of the following describes the intussuscipiens?
A. The donor loop of bowel
B. The cause of the abnormality
C. The recipient loop of bowel
D. The layer of mesenteric fat within the associated mass on computed tomography
Answers and Explanations
Question 1
A. Correct! Both the axial and coronal images demonstrate a segment of bowel and accompanying mesentery entering a downstream loop consistent with a colocolonic intussusception.
Other choices and discussion
B. Infectious colitis typically manifests as long segment bowel inflammation with a gradual transition to normal upstream or downstream bowel.
C. Bowel ischemia may be focal but is not typically masslike and would not account for the mesenteric fat within the colon on these images.
D. A Meckel’s diverticulum is a blind-ending diverticulum in the distal small bowel. A remnant of the Vitelline duct, a Meckel’s diverticulum may contain gastric mucosa and may be a source of gastrointestinal bleeding. Various gastrointestinal masses may arise within a Meckel’s diverticulum. A mass arising within a Meckel’s diverticulum might have some of the imaging features shown, but this patient’s abnormality is within the colon and appears characteristic of intussusception.
Question 2
D. Correct! Most often caused by adenocarcinoma in adults. In adults, colonic intussusception is most often caused by an underlying mass or other lead point. In children and adolescents, ileocolonic and colocolonic intussusception is most commonly spontaneous. In adults, small bowel–small bowel intussusception is also common, usually transient, and asymptomatic.
Other choices and discussion
A. Colonic intussusception is not usually self-limited in adults. Treatment of the underlying cause is usually indicated.
B. Colonic intussusception may be associated with a variety of causes, but adhesions are a less common cause than an underlying mass.
C. A benign mass such as a lipoma or leiomyoma may cause intussusception, but would be less common than adenocarcinoma.
Question 3
C. Correct! The recipient loop of bowel. It can help to remember that there are some similarities between the pronunciations of the words “intussuscipiens” and “recipient.”
Other choices and discussion
A. The donor loop of bowel is referred to as the intussusceptum.
B. The underlying cause of the abnormality is referred to as the lead point.
D. The layer of mesenteric fat does not have a special name in the terminology of intussusception.
Suggested Readings
Gollub MJ. Colonic intussusception: clinical and radiographic features. Am J Roentgenol 2011;196(5):W580–W585 Warshauer DM, Lee JKT. Adult intussusception detected at CT or MR imaging: clinical-imaging correlation. Radiology 1999;212:853–860Top Tips
Large bowel intussusception in adults is often associated with a malignancy, such as adenocarcinoma.
Small bowel intussusception in adults can be benign and transient.
The intussusceptum is the donor loop and the intussuscipiens is the receiving loop.
Essentials 7
Case
A patient presents to the emergency room with recent development of progressive abdominal pain and nausea.

Questions
1. What is the correct diagnosis?
A. Acute embolic superior mesenteric artery thrombosis
B. Acute superior mesenteric vein thrombosis
C. Portal hypertension
D. Internal hernia
2. What secondary abnormality is also present?
A. Mesenteric infarct
B. Bowel obstruction
C. Varices
D. Pneumatosis
3. Which ONE of the following statements is true for this test case diagnosis?
A. It has a low mortality.
B. It is most commonly idiopathic.
C. Resultant bowel involvement is usually segmental.
D. The inferior mesenteric vein is more commonly involved than the SMV.
Answers and Explanations
Question 1
B. Correct! Acute SMV thrombosis. The images show a filling defect within the SMV and multiple mesenteric venous branches. Always be sure to look at the mesenteric vasculature, especially when there is bowel inflammation, segmental bowel edema, mesenteric edema, or otherwise unexplained abdominal pain.
Other choices and discussion
A. The abnormality is within the SMV, rather than the artery. If unsure on a single image, scroll up and down to convince yourself you are looking at the artery or the vein.
C. Portal venous thrombosis and portal hypertension can result from SMV thrombosis. However, there is no evidence of portal hypertension on this image.
D. There is no internal hernia on these images.
Question 2
A. Correct! There is geographic mesenteric fat necrosis in the right lower quadrant, consistent with mesenteric infarct. There is also generalized edema at the root of the mesentery.
Other choices and discussion
B. There is gaseous distention of small bowel loops in the anterior abdomen, but no primary evidence of bowel obstruction.
C. Chronic mesenteric venous thrombosis can lead to varices (i.e., collateral venous channels), but well-formed collaterals are not usually present in the acute setting.
D. Pneumatosis can result from bowel ischemia in the setting of mesenteric thrombosis. However, no pneumatosis is present on the provided images.
Question 3
C. Correct! Resultant bowel involvement is usually segmental. Bowel ischemia can result from mesenteric venous thrombosis and will be limited to the segments of bowel drained by the thrombosed vein.
Other choices and discussion
A. Severe SMV thrombosis has a high mortality.
B. SMV thrombosis is rarely idiopathic, after appropriate clinical investigation. Underlying causes include hypercoagulable states, malignancy, bowel inflammation/infection, portal hypertension, recent surgery, and medications. Primary SMV thrombosis is a diagnosis of exclusion.
D. The SMV is affected more commonly than the inferior mesenteric vein.
Suggested Reading
Duran R, Denys AL, Letovanec I, Meuli RA, Schmidt S. Multidetector CT features of mesenteric vein thrombosis. RadioGraphics 2012;32(5):1503–1522Top Tips
Remember to always look at the mesenteric vasculature, especially when there is bowel inflammation, segmental bowel edema, mesenteric edema, or otherwise unexplained abdominal pain.
Scroll up and down until you are sure you know which mesenteric vessel you are looking at.
The distribution of bowel involvement with mesenteric thrombosis is usually segmental.
Essentials 8
Case
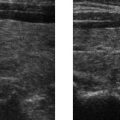
An elderly patient presents with acute left lower quadrant pain.

Questions
1. What is the most likely diagnosis?
A. Diverticulitis
B. Inflammatory bowel disease
C. Bowel ischemia
D. Epiploic appendagitis
2. What is the best next step?
A. Surgical consultation
B. Supportive therapy
C. Additional imaging
D. Colonoscopy
3. Which of the following is a potential etiology of this process?
A. Torsion
B. Luminal occlusion
C. Autoimmune
D. Infection
Answers and Explanations
Question 1
D. Correct! There is edema surrounding an oval fat lobule along the serosal margin of the descending colon, consistent with epiploic appendagitis.
Other choices and discussion
A. Acute diverticulitis is a common cause of left lower quadrant pain in adults. However, this image does not show any diverticula or peridiverticular inflammation.
B. This patient’s inflammatory changes are not centered in the bowel wall, so inflammatory bowel disease is unlikely.
C. There is no computed tomography (CT) evidence of bowel ischemia in this patient.
Question 2
B. Correct! Supportive therapy. Complications of epiploic appendagitis are rare, and supportive care alone is sufficient for management in the acute setting.
Other choices and discussion
A. Surgical consultation may be avoided by making the correct diagnosis on imaging.
C. Additional imaging is not required when characteristic CT findings are present.
D. Colonoscopy is unnecessary in epiploic appendagitis.
Question 3
A. Correct! Commonly cited etiologies of epiploic appendagitis include torsion of the appendage or thrombosis of the venous drainage.
Other choices and discussion
B. Luminal occlusion is often a cause of acute diverticulitis.
C. Autoimmune factors do not play a role in epiploic appendagitis.
D. Signs of infection such as fever and elevated white blood cell count are not usually part of the presentation.
Suggested Readings
Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendagitis and its mimics. Radiographics 2005;25(6):1521–1534Top Tips
Epiploic appendagitis is a mimic of acute inflammatory conditions such as acute appendicitis or acute diverticulitis.
On CT, there is edema surrounding an oval fat lobule along the serosal margin of the colon.
Treatment is supportive. The correct diagnosis can avoid a surgical consultation.
Essentials 9
Case
A 90-year-old man presents with acute abdominal pain. The image shows a scout X-ray prior to a fluoroscopy exam, but after a contrast computed tomography (CT).

Questions
1. Based on this image, which ONE of the following is most likely?
A. Cecal bascule
B. Cecal volvulus
C. Sigmoid volvulus
D. Toxic megacolon
2. Regarding this abnormality, which ONE of the following statements is correct?
A. The whirl sign has been described on radiographs.
B. This abnormality is the second most common type of colonic volvulus.
C. This abnormality is most commonly seen in young adulthood.
D. Chronic constipation is a risk factor.
3. Which ONE of the following is true regarding management of this abnormality?
A. There is no role for barium enema.
B. Rectal tube decompression may be therapeutic.
C. Surgical intervention is required for treatment.
D. Nasogastric decompression is indicated.
Answers and Explanations
Question 1
C. Correct! Sigmoid volvulus. The image shows a massively dilated loop of bowel emanating from the left lower quadrant, which may be difficult to appreciate initially because it is almost too large to be seen on the image. There is mild gaseous distention of the upstream colon. Of the provided options, only sigmoid volvulus would result in this appearance.
Other choices and discussion
A. Cecal bascule is an upward folding of the cecum without volvulus. The cecum must have a mesentery and lie within the peritoneum for this to occur.
B. Cecal volvulus characteristically results in a dilated loop of bowel within the central abdomen or left upper quadrant, emanating from the right abdomen. There may be resultant small bowel obstruction.
D. Colonic dilatation is expected in toxic megacolon and, indeed, severe dilatation with mural ischemia is one potential cause of toxic megacolon. However, the pattern in this test case is most consistent with sigmoid volvulus.
Question 2
D. Correct! Chronic constipation may lead to redundancy of the sigmoid colon, which can result in hypermobility and volvulus. Long-term fiber use is also a risk factor.
Other choices and discussion
A. The whirl sign has been described on CT for volvulus, but is not visible on radiographs.
B. Sigmoid volvulus is the most common type of colonic volvulus, accounting for about 70% of cases.
C. Sigmoid volvulus is most commonly seen in older adults.
Question 3
B. Correct! Placement of a decompressing rectal tube may result in resolution of the volvulus. If unsuccessful, surgical management may be required.
Other choices and discussion
A. Radiographs and CT can successfully diagnose sigmoid volvulus in the majority of patients. In equivocal cases, barium enema may contribute to the diagnosis (by demonstrating beaking of the rectosigmoid junction with obstruction to upstream flow).
C. Surgical intervention may be avoided in cases of successful rectal tube decompression.
D. Nasogastric decompression is unlikely to resolve a sigmoid volvulus.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


