SECTION VII MUSCULOSKELETAL IMAGING
Essentials 1
Case
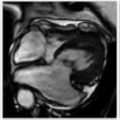
A 12-year-old male soccer player presents with knee pain.

Questions
1. What is the diagnosis?
A. Osteochondritis dissecans
B. Jumper’s knee
C. Medial collateral ligament rupture
D. Meniscal tear
E. Salter Harris type II fracture
2. Which of the following are CORRECT regarding the depicted lesion? (Select ALL that apply.)
A. Affected patients are typically under the age of 18 years.
B. Lesions most commonly affect the capitellum.
C. In the knee, these lesions are most frequently seen within the patella.
D. The proposed etiology is an injury to an epiphyseal cartilage ossification center.
E. Surgical treatment options include pinning and osteochondral grafting.
3. Which of the following is(are) a magnetic resonance imaging feature of osteochondritis dissecans instability? (Select ALL that apply.)
A. Fluid imbibition deep to the lesion
B. Cortication around the lesion
C. Fragmentation of the subchondral plate
D. Displacement or dislocation of the fragment
E. Bone marrow edema pattern
Answers and Explanations
Question 1
A. Correct! Osteochondritis dissecans (OCD) on magnetic resonance imaging appears as a focal well-circumscribed osteochondral lesion at the epiphysis, frequently occurring in the knee at the lateral aspect of the medial femoral condyle. This is also sometimes termed an osteochondral lesion.
Other choices and discussion
B. Jumper’s knee is a chronic insertional injury of the proximal attachment of the patellar tendon, presenting as thickening and increased signal within the tendon and bone marrow edema in the adjacent patella.
C. The visualized medial collateral ligament is intact.
D. No meniscal tear is demonstrated.
E. A Salter Harris type II fracture would pass across the growth plate and through the metaphysis. The growth plates and metaphyses in this patient are intact.
Question 2
A. Correct! Patients with OCD lesions tend to be young (under 18 years) and are twice as likely to be male.
D. Correct! Although the exact cause is unknown, OCD is thought to be secondary to an injury of an ossification center in the epiphyseal cartilage.
E. Correct! Surgical treatment options for unstable OCD lesions include microfracture, pinning of the osteochondral lesion, and osteochondral grafting (autograft or allograft).
Other choices and discussion
B. OCD most commonly affects the knee. It can also be seen in the talar dome of the ankle and in the capitellum of the elbow.
C. In the knee, osteochondral lesions are most frequently seen in the lateral aspect of the medial femoral condyle (70%). Lateral condylar lesions are the next most frequent (10 to 20%). Patellar lesions account for 5 to 10% of cases, and trochlear lesions are rarely seen.
Question 3
A. Correct! A T2 hyperintense (fluid intensity or granulation tissue intensity) rim surrounding an OCD lesion suggests instability in adults. However, because osteochondral lesions frequently heal with conservative management in juvenile patients, the criteria are stricter, and this rim must be fluid signal. The presence of cysts (even one) surrounding an OCD lesion in an adult is consistent with instability, but in a juvenile patient, the cysts should be > 5 mm in size and multiple in number to suggest instability. But even in the latter scenario, some lesions will go on to heal without surgical intervention.
B. Correct! Low-signal intensity rim or cortication around the lesion suggests instability. This would have a similar appearance to chronic ununited fractures elsewhere in the body, with the low signal cortication seen on the opposing surfaces of both the lesion and the parent bone.
C. Correct! Fragmentation of the subchondral plate suggests instability.
D. Correct! Displacement or dislocation of the fragment suggests instability.
Incorrect choice and discussion
E. A bone marrow edema pattern may be seen within the lesion or the donor site in the setting of an OCD. However, this alone is not a sign of instability.
Suggested Readings
Chang GH, Paz DA, Dwek JR, Chung CB. Lower extremity overuse injuries in pediatric athletes: clinical presentation, imaging findings, and treatment. Clin Imaging 2013;37(5):836–846 McKay S, Chen C, Rosenfeld S. Orthopedic perspective on selected pediatric and adolescent knee conditions. Pediatr Radiol 2013;43(Suppl 1):S99–106 Moktassi A, Popkin CA, White LM, Murnaghan ML. Imaging of osteochondritis dissecans. Orthop Clin North Am 2012;43(2):201–211, v–viTop Tips
OCD lesions are most frequently seen in patients under 18 years and affect males more than females.
OCD is most commonly seen in the knee, at the lateral aspect of the medial femoral condyle.
Signs of OCD instability on magnetic resonance imaging include a fluid signal rim deep to the lesion, cortication of the fragment and the adjacent donor site, and displacement or dislocation of the lesion.
Essentials 2
Case
A previously healthy 48-year-old man presents with trauma and right foot pain.

Questions
1. Which ONE of the following is the correct diagnosis?
A. Second metatarsal base fracture
B. Lisfranc fracture-dislocation
C. Neuropathic joint
D. Chopart joint dislocation
E. Midfoot sprain
2. How many components make up the injury in this case?
A. One
B. Two
C. Three
D. Four
E. Six
3. What is the best next step in management for this patient?
A. Surgical fixation
B. Closed reduction
C. Placing the patient in a walking boot
D. Repeat radiographs in 10 to 14 days
E. Ultrasound
Answers and Explanations
Question 1
B. Correct! This is a Lisfranc fracture-dislocation. Offset of the second tarso-metatarsal (TMT) joint is the result of a Lisfranc ligament injury. The Lisfranc ligament runs from the second metatarsal base to the medial cuneiform. Lisfranc fracture-dislocations are divided into homolateral, in which the first through fifth metatarsals are displaced laterally, and divergent, in which the second through fifth metatarsals are displaced laterally but the first metatarsal is displaced medially. Complete Lisfranc fracture-dislocations involve all five metatarsals. In the test case, the first metatarsal base is fractured and dislocated medially. This is an example of an incomplete divergent Lisfranc fracture-dislocation. Disruption of the Lisfranc ligament typically occurs with midfoot plantar flexion in low impact trauma and with direct force in high impact trauma (i.e., motor vehicle accident).
Other choices and discussion
B. The second metatarsal base is not fractured.
C. This patient has an unremarkable past medical history and presents with an acute injury, making neuropathy unlikely. Note that neuropathy can predispose to a Lisfranc ligament injury. This is often seen in diabetic patients, may be clinically silent, and may result in midfoot arthritis and pes planus.
D. The Chopart joint refers to the calcaneocuboid and talonavicular joints. These are normal in the test case.
E. A midfoot sprain refers to Lisfranc ligament sprain without disruption of the second TMT joint. The test case demonstrates a more serious injury.
Question 2
C. Correct! The Lisfranc ligament has three components: dorsal, interosseous, and plantar. All connect the base of the second metatarsal to the medial cuneiform. The dorsal band is the weakest, explaining the frequent dorsal dislocation of the second metatarsal base with a Lisfranc ligament rupture. Weight-bearing views of the foot are very useful in depicting this dorsal dislocation.
Question 3
A. Correct! A Lisfranc fracture-dislocation or Lisfranc ligament injury that is unstable or displaced can lead to osteoarthritis and midfoot collapse if not surgically repaired in anatomic alignment.
Other choices and discussion
B. The more conservative treatment of closed reduction puts the patient at a greater risk for subsequent morbidity.
C. The more conservative treatment of placing the patient in a walking boot puts the patient at a greater risk for subsequent morbidity.
D. Repeating the radiograph is unlikely to add useful information, as the diagnosis is made on the initial radiographs.
E. Ultrasound may detect a tear of the Lisfranc ligament. However, because the radiograph already shows a Lisfranc fracture-dislocation, ultrasound is not needed. Some surgeons use computed tomography or magnetic resonance imaging for preoperative planning and to assess for additional radiographically occult fractures that can accompany Lisfranc injuries.
Suggested Readings
Crim J. MR imaging evaluation of subtle Lisfranc injuries: the midfoot sprain. Magn Reson Imaging Clin N Am 2008;16(1): 19–27 Siddiqui NA, Galizia MS, Almusa E, Omar IM. Evaluation of the tarsometatarsal joint using conventional radiography, CT, and MR imaging. Radiographics 2014;34(2):514–531Top Tips
In both homolateral and divergent Lisfranc injuries, the second through fifth metatarsals are displaced laterally. In divergent, the first metatarsal is displaced medially. In homolateral, the first metatarsal is displaced laterally (i.e., remains congruent with the other metatarsals).
A Lisfranc injury can be easily missed on plain film, especially if the foot is imaged without weight bearing. Weight-bearing views are very important if there is concern for a midfoot injury. Even subtle offset of the second TMT joint suggests a Lisfranc injury.
The Lisfranc ligament runs from the second metatarsal base to the medial cuneiform.
Essentials 3
Case
A 27-year-old woman presents with thumb pain following an acute injury.

Questions
1. Which diagnosis do the radiographs demonstrate?
A. Ulnar collateral ligament injury
B. Radial collateral ligament injury
C. Pulley injury
D. Extensor tendon injury
E. Flexor tendon injury
2. Which ONE of the following choices is NOT an appropriate step in the management of the injury shown above?
A. Magnetic resonance imaging
B. Surgical fixation
C. Repeat radiographs with stress views
D. Conservative management
E. Ultrasound
3. What is the mechanism of injury in this case?
A. Hyperadduction
B. Hyperabduction
C. Axial loading
D. Hyperextension
E. Hyperflexion
Answers and Explanations
Question 1
A. Correct! A small bony fragment adjacent to the ulnar base of the thumb proximal phalanx is seen. This indicates an ulnar collateral ligament (UCL) avulsion fracture. This has been classically referred to as a “gamekeeper’s thumb,” referencing chronic UCL injuries in patients who repetitively broke the necks of small game (rabbits). Today, this injury is most commonly seen with skiers (although “skier’s thumb” is considered more of an acute injury by some). The fracture fragment in this case is displaced and rotated. The thumb metacarpophalangeal joint may be in valgus angulation with radial subluxation of the proximal phalanx.
Other choices and discussion
B. The radial collateral ligament attaches to the radial aspect of the proximal phalanx and, if injured, results in an avulsion fragment at that site and/or ulnar subluxation of the proximal phalanx.
C. Pulley injuries rarely result in avulsion fractures and therefore are typically radiographically occult.
D. An extensor tendon injury is not present in the test case. A dorsal avulsion fracture and a fixed flexion deformity could represent an extensor tendon injury.
E. A flexor tendon injury is not present in the test case. A volar avulsion fracture and a fixed extension deformity could represent a flexor tendon injury.
Question 2
C. Correct! Stress views should never be performed in patients with a gamekeeper’s thumb, as stress views can actually create a Stener lesion and transform a nonsurgical injury into a surgical injury. A Stener lesion is present when the torn UCL is abnormally displaced over the adductor aponeurosis/adductor pollicus tendon. This alignment will prevent normal ligament healing, and therefore a Stener lesion requires surgical fixation.
Other choices and discussion
A. Magnetic resonance imaging (MRI) is helpful in evaluating the extent of injury to the UCL and in assessing for a possible Stener lesion. A UCL injury can often be very subtle or occult on initial radiographs.
B. Surgical fixation is required in the presence of a Stener lesion. In this case, the displaced and rotated fracture fragment is concerning for the presence of a Stener lesion. This was subsequently proven surgically, as the patient underwent surgical reduction and fixation of the UCL and avulsion fragment.
D. Conservative management (immobilization and pain control) is often sufficient to treat a nondisplaced UCL tear. However, when a Stener lesion is present, or when conservative management has failed, surgical fixation is required.
E. Like MRI, ultrasound is helpful in evaluating the extent of injury to the UCL and in assessing for a possible Stener lesion. Musculoskeletal ultrasound is often a dynamic examination, but for this indication, dynamic imaging should either be avoided or performed very carefully to avoid causing a Stener lesion.
Question 3
B. Correct! The UCL is injured when the thumb undergoes extreme hyperabduction. Gamekeeping, skiing, and break dancing have all been implicated as risk factors.
Other choices and discussion
A. A hyperadduction injury would not injure the UCL. (An injury to the radial collateral ligament would be more likely with that mechanism.)
The other mechanisms would not typically account for an injury to the UCL.
Suggested Readings
Clavero JA, Alomar X, Monill JM, Esplugas M, Golano P, Mendoza M, Salvador A. MR imaging of ligament and tendon injuries of the fingers. Radiographics 2002;22:237–256 Hinke DH, Erickson SJ, Chamoy L, Timins ME. Ulnar collateral ligament of the thumb: MR findings in cadavers, volunteers, and patients with ligamentous injury (gamekeeper’s thumb). Am J Roentgenol 1994;163:1431–1434 Hirschmann A, Sutter R, Scweizer A, Pfirrmann CW. MRI of the thumb: anatomy and spectrum of findings in asymptomatic volunteers. Am J Roentgenol 2014;202:819–827Top Tips
Gamekeeper’s (or skier’s) thumb describes a hyperabduction injury to the UCL of the thumb metacarpophalangeal joint. Ultrasound and MRI are both quite useful in this assessment.
A Stener lesion occurs when the torn UCL is displaced above the adductor aponeurosis/adductor pollicus tendon. This requires surgical fixation.
Radiographic stress views should not be performed, and extreme care should be taken during dynamic maneuvers with ultrasound to avoid causing a Stener lesion.
Essentials 4
Case
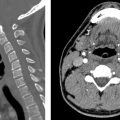
A 53-year-old man presents with stiffness, neck and back pain, and no other systemic symptoms.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Psoriatic arthritis
B. Diffuse idiopathic skeletal hyperostosis
C. Reactive arthritis
D. Ankylosing spondylitis
E. Inflammatory bowel disease arthritis
2. What is the primary site of disease in this disorder?
A. Bone
B. Synovial membrane
C. Enthesis
D. Cartilage
E. Ligament
3. What is the most common location of a Romanus lesion?
A. Cervical spine
B. Midthoracic spine
C. Thoracolumbar junction
D. Lower lumbar spine
E. SI joints
Answers and Explanations
Question 1
D. Correct! The sacroiliac (SI) joints are fused bilaterally, consistent with chronic bilateral sacroiliitis. The cervical spine radiograph shows multilevel thin, bridging syndesmophytes, consistent with a “bamboo spine.” This presentation is typical of ankylosing spondylitis, a seronegative spondyloarthropathy with a strong HLA-B27 antigen association. “Seronegative” refers to the absence of rheumatoid factor.
Other choices and discussion
A. Psoriatic arthritis is associated with bulky paravertebral ossification, not thin flowing syndesmophytes, as in the test case. Psoriatic arthritis is commonly associated with asymmetric bilateral sacroiliitis, although in chronic cases, sacroiliitis may become more symmetric.
B. Diffuse idiopathic skeletal hyperostosis is associated with multilevel bulky ossification of the paraspinal ligaments, not thin flowing syndesmophytes. Diffuse idiopathic skeletal hyperostosis is usually considered an incidental finding and is not associated with sacroiliitis, although the SI joints can be fused superiorly by bulky bridging bone, similar in appearance to that seen in the spine.
C. Reactive arthritis (formerly known as Reiter syndrome) is typically associated with asymmetric bilateral sacroiliitis, although in chronic cases, sacroiliitis may become more symmetric. In the spine, reactive arthritis is associated with bulky paravertebral ossification, not thin flowing syndesmophytes.
E. Inflammatory bowel disease is associated with arthropathy, and its radiographic appearance can be similar to that of ankylosing spondylitis. However, because this patient had no gastrointestinal symptoms, inflammatory bowel disease arthritis is unlikely.
Question 2
C. Correct! The enthesis is the primary site of disease in ankylosing spondylitis and represents the connective tissue between a tendon or ligament and bone. Because the SI joints are predominantly lined with fibrocartilage and with very little synovial tissue, these joints can be thought of as entheses, explaining their characteristic involvement in spondyloarthropathies such as ankylosing spondylitis. Chronic inflammation of an enthesis can lead to subsequent ankylosis. Patients with ankylosis are at an increased risk for developing fractures.
Sacroiliitis is usually the first site involved by ankylosing spondylitis. This disease affects the spine and hips, and can also affect the shoulders, knees, hands, and the lung parenchyma (with apical predominant fibrobullous changes).
Other choices and discussion
B. The synovial membrane is the primary site of disease in rheumatoid arthritis, not ankylosing spondylitis.
The other choices are incorrect.
Question 3
C. Correct! The thoracolumbar junction is the most common site of a Romanus lesion. A Romanus lesion is a focal inflammatory erosive area along the anterior superior or anterior inferior margin of a vertebral body and can be seen early in the course of spondyloarthropathies. With magnetic resonance imaging, they show focal short tau inversion recovery hyperintensity during active inflammation. Later, these lesions may become sclerotic as they heal, leading to the “shiny corner” sign. They can also leave behind postinflammatory fatty marrow (without short tau inversion recovery hyperintensity).
Discussion
Regarding the SI joint, there are several mimics of true sacroiliitis. Hyperparathyroidism can cause erosion and mimic bilateral sacroiliitis. Osteitis condensens ilii is not a true sacroiliitis. This refers to benign sclerosis of the ilium as it borders the SI joint. This is often triangular in shape. Diagnosis can be made when this finding is seen with a lack of involvement of the adjacent sacrum and preservation of the SI joint space. This is usually asymptomatic.
Only the lower half of the SI joint represents a true diarthrodial joint. Scrutinize the lower half of the SI joint carefully when assessing for arthropathy.
Suggested Readings
Jang JH, Ward MM, Rucker AN, Reveille JD, Davis Jr JC, Weisman MH, Learch TJ. Ankylosing spondylitis: patterns of radiographic involvement—a re-examination of accepted principles in a cohort of 769 patients. Radiology 2011;258:192–198 Kim NR, Choi J-Y, Hong SH, Jun WS, Lee JW, Choi J-A, Kang HS. “MR corner sign”: value for predicting presence of ankylosing spondylitis. Am J Roentgenol 2008;191:124–128 Lacout A, Rousselin B, Pelage J-P. CT and MRI of spine and sacroiliac involvement in spondyloarthropathy. Am J Roentgenol 2008;191:1016–1023Top Tips
Ankylosing spondylitis is associated with symmetric and bilateral sacroiliitis and multilevel bridging syndesmophytes in the spine, leading to ankylosis and the characteristic “bamboo spine” appearance. A spine with ankylosis is at an increased risk of fracture.
Unilateral sacroiliitis is infection until proven otherwise.
Differential diagnoses of bilateral and symmetric sacroiliitis: inflammatory bowel disease, ankylosing spondylitis. Differential diagnoses of bilateral but asymmetrical sacroiliitis: rheumatoid arthritis, gout, psoriatic arthritis, reactive (Reiter arthritis), and osteoarthritis.
Essentials 5
Case
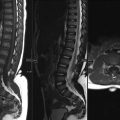
A 42-year-old man presents with back pain.

Questions
1. Which underlying condition is likely present?
A. Paget disease
B. Hyperparathyroidism
C. Sickle cell disease
D. Osteopetrosis
E. Renal osteodystrophy
2. What is the cause of the endplate depression in the test case?
A. Trauma
B. Infarction
C. Infection
D. Surgery
E. Hemorrhage
3. Which of the following are musculoskeletal manifestations of sickle cell disease? (Select ALL that apply.)
A. Osteomyelitis
B. Growth disturbance
C. Extramedullary hematopoiesis
D. Malignancy
E. Skin ulceration
Answers and Explanations
Question 1
C. Correct! The central endplate depression seen in multiple vertebral bodies is typical of sickle cell disease. The biconcave endplates in the test case result in a “fish mouth” appearance. The more characteristic “H shaped” or “Lincoln log” vertebrae may be seen later as the endplate infarcts progress.
Other choices and discussion
A. Paget disease in the spine is characterized by dense sclerosis and overgrowth of the vertebral body.
B. Hyperparathyroidism in the spine produces transverse vertebral body endplate sclerosis, likened to a rugby or “rugger” jersey. If there are superimposed endplate insufficiency fractures, the vertebrae may take on a fish mouth appearance. No endplate sclerosis is present in the test case, however.
D. Osteopetrosis in the spine causes dense vertebral body endplate sclerosis, resulting in a “sandwich” vertebra.
E. Renal osteodystrophy in the spine results in a similar appearance to that of hyperparathyroidism.
Question 2
B. Correct! The vertebral body central endplate depression in sickle cell disease is caused by bone infarcts.
Discussion
Sickle-cell disease is an autosomal recessive condition characterized by abnormally shaped red blood cells. Its impact is extensive throughout the body, and it results in considerable morbidity and mortality. Typical radiographic findings include the vertical “hair-on-end” appearance of the calvarium, H-shaped or “fish-mouth” vertebrae, diffuse osteopenia, and coarsening of the trabeculae in the long bones.
Associated persistence of red marrow in the long bones and additional sites of red marrow reconversion are seen on magnetic resonance imaging. Marrow expansion is also detected on bone scintigraphy. Patients with sickle cell disease are predisposed to both infarcts and osteomyelitis.
Question 3
A. Correct! Patients with sickle cell disease have an increased incidence of osteomyelitis and septic arthritis because of bone infarcts and hyposplenism. Hyposplenism reduces the body’s ability to eradicate certain bacteria. Salmonella infections are particularly common with sickle cell patients.
B. Correct! Impaired growth occurs subsequent to bone infarcts, which affect the epiphyses and growth plates.
C. Correct! Although extramedullary hematopiesis occurs more in thalassemia and hemolytic anemias, it can also be seen with sickle cell disease, resulting in osseous expansion and soft tissue masses in the chest, adrenal glands, and skin.
E. Correct! Sickle cell disease causes venous stasis and tissue hypoxia, which produces skin ulceration, particularly over bony prominences.
Incorrect choice and discussion
D. There is no conclusive evidence for an increased risk of musculoskeletal malignancy with sickle cell disease. Renal medullary cancer, a rare and aggressive neoplasm of the kidney, is associated with sickle cell trait.
Suggested Readings
Ejindu VC, Hine AL, Mashayekhi M, Shorvon PJ, Misra RR. Musculoskeletal manifestations of sickle cell disease. Radiographics 2007;27(4):1005–1021 Martinoli C, Bacigalupo L, Forni GL, Balocco M, Garlaschi G, Tagliafico A. Musculoskeletal manifestations of chronic anemias. Semin Musculoskelet Radiol 2011;15(3):269–280Top Tips
Sickle cell disease predisposes to hematogenous osteomyelitis, and Salmonella is the most common pathogen. Prominent red marrow reconversion can be seen in unusual locations, and differentiation from hematogenous osteomyelitis is sometimes difficult.
Using a patient’s younger age and the presence of H-shaped vertebra on a chest radiograph may help to differentiate a sickle cell patient in crisis from a patient with congestive heart failure.
Sickle cell disease predisposes to multifocal bone infarctions. In the spine, “H-shaped” vertebrae are fairly unique to sickle cell disease, whereas “fish mouth” vertebrae are less specific and can be seen in other conditions including osteoporosis, renal osteodystrophy, and thalassemia.
Essentials 6
Case
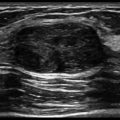
A 43-year-old woman presents with shoulder pain.

Questions
1. Which ONE of the following is the correct diagnosis?
A. Greater tuberosity fracture
B. Calcific tendinosis
C. Frozen shoulder
D. Humeral head chondroblastoma
E. Humeral neck fracture
2. Which ONE of these is the MOST common site for the test case finding?
A. Rotator cuff
B. Elbow
C. Knee
D. Achilles tendon
E. Thumb
3. Which of the following is(are) true regarding rotator cuff calcific tendinosis? (Select ALL that apply.)
A. Painful disease is often associated with subdeltoid bursitis.
B. The main treatment option is surgical resection.
C. Doppler hyperemia correlates with pain.
D. There are formative, resting, and resorptive phases.
E. Calcific deposits can erode into bone.
Answers and Explanations
Question 1
B. Correct! There is focal globular soft tissue mineralization in the region of the rotator cuff insertion, consistent with hydroxyapatite crystal deposition, or calcific tendinosis.
Other choices and discussion
A. A greater tuberosity fracture would have bone matrix, not amorphous calcium as is shown in the test case.
C. A frozen shoulder (or adhesive capsulitis) is characterized by thickening and contraction of the joint capsule and synovium of the shoulder. The plain film is typically normal. Magnetic resonance imaging sometimes shows capsular thickening and high signal in the axillary recess, and intermediate signal in the rotator interval.
D. A chondroblastoma is typically a well-defined lucent lesion seen in young patients (younger than age 20 years), localized to the epiphysis of a long bone. The test case demonstrates several small lucent lesions with sclerotic rims in the humeral head. However, these are typical of benign enthesopathic intraosseous cysts.
E. There is no humeral neck fracture. There is a mild humeral head osteophyte formation, which can sometimes mimic a fracture.
Question 2
A. Correct! Calcific tendinosis most commonly affects the shoulders, and in particular the rotator cuff. These calcific deposits may also occur in the wrists, elbows, hands, hips, knees, and feet.
Within the rotator cuff, the distribution breakdown is as follows: supraspinatus (80%), infraspinatus (15%), and subscapularis (5%).
Question 3
A. Correct! Calcific deposits can shed into the overlying subdeltoid bursa, causing inflammation and pain, which may be severe.
C. Correct! Both Doppler hyperemia and subdeltoid bursal distention correlate with pain in calcific tendinosis.
D. Correct! There are formative, resting, and resorptive phases. During the formative phase, calcium crystals coalesce within the tendon to form a calcific focus. During the resting phase, fibrocartilaginous tissue encapsulates the calcific focus. During the resorptive phase, there is spontaneous resorption of the calcium, which generates an inflammatory response that is often characterized by an acute pain syndrome and limited range of motion.
E. Correct! During the resorptive phase, the calcium is shed into the overlying subdeltoid bursa and can erode into bone, causing inflammation. On magnetic resonance imaging, these inflammatory changes can appear very aggressive and raise suspicion for infection or malignancy. Bony erosion can also appear aggressive on computed tomography. Ultrasound and radiographs are recommended for the imaging evaluation of calcific tendinosis, given the typical appearance on these modalities and the relatively low cost.
Other choice and discussion
B. The main treatment is NOT surgical resection. Treatment options for rotator cuff calcific tendinosis include ultrasound-guided aspiration/lavage and subacromial-subdeltoid bursal corticosteroid injection. These have a high treatment success rate. Refractory cases may undergo surgical resection, but this is uncommon.
Suggested Readings
Bureau NJ. Calcific tendinopathy of the shoulder. Semin Musculoskelet Radiol 2013;17(1):80–84 Le Goff B, Berthelot JM, Guillot P, Glemarec J, Maugars Y. Assessment of calcific tendonitis of rotator cuff by ultrasonography: comparison between symptomatic and asymptomatic shoulders. Joint Bone Spine 2010;77:258–263 Levy O. Ultrasound-guided barbotage in addition to ultrasound-guided corticosteroid injection improved outcomes in calcific tendinitis of the rotator cuff. J Bone Joint Surg Am 2014;96:335Top Tips
The most common site of calcific tendinosis (or hydroxyapatite crystal deposition) is the rotator cuff, but this entity can affect other tendons as well, such as the gluteal insertions and the hamstring origins.
Inflammation related to calcific tendinosis can contribute to extreme shoulder pain, prompting a visit to the emergency department or urgent care clinic for evaluation.
Calcific tendinosis eroding into bone can have an aggressive appearance on computed tomography and magnetic resonance imaging, and mimic a malignant bone lesion.
Essentials 7
Case
A 56-year-old man presents with anterior knee pain and swelling.

Questions
1. Which ONE of the following is the most likely diagnosis?
A. Gout
B. Quadriceps tendon tear
C. Enthesopathy
D. Rheumatoid arthritis
E. Osteomyelitis
2. Which of the following is the MOST common site of involvement of this entity?
A. Hip joint
B. Medial aspect of the first metatarsal head
C. Lumbar spine
D. Radiocarpal joint
E. Glenohumeral joint
3. Regarding gout, which of the following are correct? (Select ALL that apply.)
A. Marginal osseous erosions with sclerotic margins and overhanging edges occur late in the disease process.
B. Sonographic features of gout include joint effusion, as well as echogenic deposits in the joint fluid, the synovium, and/or the cartilage surface.
C. Tophi are always intra-articular.
D. Use of urate lowering therapy increases the sensitivity and specificity of dual energy computed tomography (CT) for the diagnosis of gout.
E. Tophi usually have the typical T1 hypointense, T2 hyperintense appearance of most masses.
Answers and Explanations
Question 1
A. Correct! Magnetic resonance images reveal an anterior patellar cortex osseous erosion, with defined sclerotic margins and overhanging edges, giving the appearance of a “rat-bite.” The soft tissue material in the bed of the erosion is of intermediate signal. These findings are typical for a gouty tophus.
Other choices and discussion
B. A torn quadriceps tendon at the distal-most insertion on the patella would have the abnormality centered at the tendon (with discontinuity of fibers and intrinsic high signal), rather than centered at the bone, as in this case. If present, a complete quadriceps tendon tear would retract the patella in a distal direction (“patella baja”).
C. Patellar enthesopathy is seen as osseous proliferation or spurring at the quadriceps or patellar attachments. It involves inflammation at sites where ligaments, tendons, or joint capsules attach to the bone. Enthesopathy would not be associated with erosions.
D. Erosions associated with rheumatoid arthritis usually occur in the bare areas of synovial joints and do not typically demonstrate the sclerotic margins or overhanging edges seen in gout. Synovitis is the earliest abnormality to appear with rheumatoid arthritis, which is not demonstrated in this case.
E. The lack of an adjacent soft tissue ulcer makes infection less likely than gout. Additionally, an acute infection is unlikely to produce an intraosseous lesion with such well-defined margins. However, infection in soft tissue often affects adjacent bone—for example, direct extension from a foreign body is possible—and infection would be a diagnostic consideration.
Question 2
B. Correct! Approximately 50% of the cases of gout occur at the medial aspect of the first metatarsal head. Gout is found in the ankles (Achilles), feet (intertarsal joints), wrists (carpometacarpal compartment), in entheses around the knees (patellar and popliteus tendons), shoulders, and sacroiliac joints. Bilateral olecranon effusions may be seen and are a clue to the correct diagnosis.
All other choices are incorrect.
Question 3
A. Correct! Marginal osseous erosions with sclerotic margins and overhanging edges occur late in the disease process. Most early presentations of gout have normal plain films.
B. Correct! Sonographic features of gout include joint effusion, as well as echogenic deposits in the joint fluid, the synovium, and/or the cartilage surface. Ultrasound is very sensitive for detecting joint fluid and is also capable of visualizing fine echogenic deposits.
Other choices and discussion
C. Tophaceous deposits are not restricted to intra-articular locations.
D. Dual energy CT has demonstrated a sensitivity and specificity of up to 100% and 95%, respectively, for the diagnosis of gout. However, frequent use of urate lowering therapy may decrease the sensitivity for diagnosing gout with dual energy CT.
E. Tophi have usually do not the typical T1 hypointense, T2 hyperintense appearance of most masses. On magnetic resonance imaging, tophi are usually T1 and T2 isointense and demonstrate prominent enhancement. There may be variable signal, depending on the amount of calcium.
Suggested Readings
Girish G, Glazebrook KN, Jacobson JA. Advanced imaging in gout. Am J Roentgenol 2013;201(3):515–525 O’Connor PJ. Crystal deposition disease and psoriatic arthritis. Semin Musculoskelet Radiol 2013;17(1):74–79Top Tips
The classic radiographic features of gouty erosions are late disease manifestations and include focal intraosseous defects with sclerotic margins and overhanging edges. Because of earlier diagnosis and treatment today, many cases of gout will have a normal radiograph.
With gout, there is preservation of the joint space until late in the disease, unlike osteoarthritis. With gout, there is absence of periarticular demineralization, unlike rheumatoid arthritis.
Tophi on magnetic resonance imaging are variable but often T1 and T2 isointense with prominent enhancement. Dual energy CT is also useful in detecting uric acid crystals and diagnosing gout.
Essentials 8
Case
A 45-year-old man presents with knee pain and clicking.

Questions
1. Which ONE of the following conditions is both demonstrated in this case and predisposes to knee instability?
A. Osteophytes
B. Discoid meniscus
C. Medial collateral ligament tear
D. Bone bruise
E. Anterior cruciate ligament tear
2. Regarding this disorder, which of the following are correct? (Select ALL that apply.)
A. Hypermobile
B. Most frequently affects the lateral meniscus
C. Acquired condition
D. Increases the risk of meniscal degeneration
E. Rarely bilateral
3. Which of the following is(are) correct regarding the magnetic resonance imaging (MRI) appearance of a discoid meniscus? (Select ALL that apply.)
A. Demonstrates continuity of the anterior and posterior horns on three or more contiguous 5-mm thick sagittal images
B. Occupies > 50% of the lateral femorotibial joint space
C. Often demonstrates diffusely increased meniscal signal intensity
D. Presence of a meniscal tear increases the ability of MRI to accurately diagnose a discoid meniscus
E. Arthroscopic treatment may include saucerization and debulking
Answers and Explanations
Question 1
B. Correct! Discoid meniscus (which is seen in the lateral meniscus of the test case) is thought to represent a multifactorial congenital condition in which the center of the meniscus contains extra meniscal tissue. Despite the extra meniscal tissue, the meniscus is more prone to injury than a normal meniscus. A discoid meniscus may be fully or partially discoid, both of which produce an abnormally thickened and enlarged morphology. A discoid meniscus is often hypermobile, predisposed to injury, and places the patient at an increased risk for knee instability.
Other choices and discussion
A. Osteophytes form as the result of osseous remodeling, typically seen in response to cartilage loss in a joint. If large enough, osteophytes may result in soft tissue impingement or a clicking sensation. Osteophytes would not predispose to joint instability.
C. The medial collateral ligament is slightly thickened, but there is no discontinuity of fibers, no adjacent inflammation, and no evidence for a tear. The thickening in this case may be the result of nonacute altered weight bearing or prior sprain.
D. No obvious bone bruise is present, although fluid-sensitive sequences would be needed to exclude this type of microtrabecular injury. Even if present, a bone bruise would be painful but would not predispose to joint instability.
E. An anterior cruciate ligament tear would predispose the knee to instability, but the anterior cruciate ligament appears intact based on the coronal image.
Question 2
A. Correct! The discoid meniscus is hypermobile and may be devoid of peripheral attachments, predisposing to injury.
B. Correct! The incidence of discoid meniscus is much higher for the lateral meniscus than for the medial meniscus.
D. Correct! There are decreased collagen fibers and loss of normal collagen orientation in a discoid meniscus, and mucoid degeneration is common. Additionally, discoid menisci are more susceptible to injury than normal menisci, as their abnormal shape and thickness results in increased biomechanical stress.
Other choices and discussion
C. Discoid meniscus is a multifactorial congenital condition, not acquired.
E. A discoid meniscus is often bilateral (up to 50%).
Question 3
A. Correct!
B. Correct! This is seen on the coronal images.
C. Correct! Discoid menisci are predisposed to degeneration, which presents as diffuse intrasubstance high signal on MRI.
E. Correct! When discoid menisci are torn or unstable, surgical treatment is considered. Arthroscopic treatment commonly includes saucerization and debulking of the meniscus to restore a normal shape and to stabilize the meniscus, if there is meniscal instability upon probing.
Other choice and discussion
D. The presence of a meniscal tear disrupts the standard meniscal signal and morphology, and somewhat decreases the ability of MRI to accurately diagnose a discoid meniscus.
Suggested Readings
Francavilla ML, Restrepo R, Zamora KW, Sarode V, Swirsky SM, Mintz D. Meniscal pathology in children: differences and similarities with the adult meniscus. Pediatr Radiol 2014;44(8):910–925 McKay S, Chen C, Rosenfeld S. Orthopedic perspective on selected pediatric and adolescent knee conditions. Pediatr Radiol 2013;43(Suppl 1):S99–106Top Tips
Discoid meniscus most commonly affects the lateral meniscus (incidence ratio is 10:1 for lateral:medial meniscus).
A total of 2% of the population has a discoid lateral meniscus.
Discoid menisci are predisposed to degeneration, tear, and subsequent joint instability.
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


