CHAPTER 14 Sella Turcica and Pituitary Gland
The sellar and parasellar regions comprise the sella turcica, the pituitary gland, and the adjoining soft tissues and bone. The parasellar structures include the sphenoidal sinus and adjoining central skull base, the paired cavernous sinuses and adjoining venous sinuses, the cavernous and supraclinoid segments of the internal carotid arteries, the circle of Willis, the optic nerves and chiasm, the infundibulum and hypothalamus, the anterior recesses of the third ventricle, and the suprasellar subarachnoid space (suprasellar cistern). The sellar/parasellar region is an important junction for neurovascular, ophthalmologic, and endocrinologic structures.
The sella turcica (L., “Turkish saddle”) forms as a spherical depression within the dorsal surface of the sphenoid bone. The sella and pituitary gland are related superiorly to the suprasellar cistern, the supraclinoid segments of the internal carotid arteries and circle of Willis, the pituitary stalk (infundibulum), the hypothalamus and anterior recesses of the third ventricle, the optic nerves, the optic chiasm, and the optic tracts. The sella is related laterally, on each side, to the paired cavernous sinuses, the cavernous segments of the internal carotid arteries, and cranial nerves (CN) III, IV, V1 and V2, and VI). It is related posteriorly to the basilar artery in the prepontine and interpeduncular cisterns and posteroinferolaterally to Meckel’s cave, CN V, and the trigeminal ganglion. Directly inferiorly, the sella and pituitary gland are related to the sphenoidal sinus and, through that, to the nasopharynx. Dural reflections from the diaphragma sellae overlie the sella and the walls of the cavernous sinuses laterally.1–3 Surgical access to the sella is limited by the surrounding vital structures, making the preferred surgical routes to sellar lesions the transsphenoidal approach through the sphenoidal sinus and the subfrontal approach along the floor of the anterior cranial fossa.4,5 Familiarity with the anatomy and surgical landmarks of this region will permit proper display and appreciation of regional pathologic processes to facilitate diagnosis and medical/surgical management of sellar-parasellar disease.
ANATOMY
Gross Anatomy
Sphenoid Bone, Sphenoidal Sinus, and Anatomic Relationships
Sphenoid Bone
The sphenoid bone lies within the central skull base. When viewed anteriorly, it displays a central body and numerous projections, like a bat with outstretched wings (Figs. 14-1 to 14-3). Two lesser wings of the sphenoid bone project upward from the superolateral surfaces of the body on each side. Two greater wings of the sphenoid bone originate from the inferior portion of the sphenoid body and also project superolaterally, inferior to the lesser wings. Paired gaps between the lesser wings above and the greater wings below are designated the superior orbital fissures. Paired pterygoid processes arise from the undersurface of the sphenoid body on each side, project inferiorly, and flare outward as paired medial and lateral pterygoid plates. Cranial nerves (CN) III, IV, V1, and VI pass through the superior orbital fissure (Fig. 14-4). The posterior frontal lobes, olfactory tracts, and gyri recti rest on the smooth dorsal surfaces of the lesser sphenoid wings and planum sphenoidale. The lateral margin of each lesser wing forms the sphenoid ridge. On each side, the sphenoid ridges project upward into the sylvian fissure between the undersurface of the frontal lobe and the superior surface of the temporal lobe. The basilar artery and brain stem lie posterior to the clivus (Figs. 14-5 and 14-6).
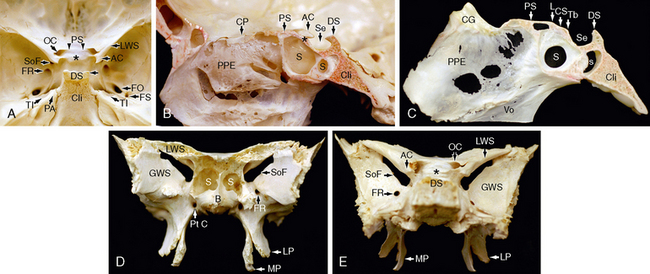
FIGURE 14-1 Gross anatomy of the skull base and sphenoid bone. Three specimens of dried skulls. A, Specimen 1. View of the sella turcica (Se) from above and behind. B and C, Specimen 2. Sagittal sections through the sella and parasellar region. D and E, Specimen 3. Anterior surface (D) and posterior surface (E) of an isolated sphenoid bone. The sphenoid bone contains the pneumatized sphenoidal sinus (S) and gives rise to multiple bony processes. These include the lesser (L) and greater (G) sphenoid wings (SW), the anterior clinoid processes (AC) at the medial ends of the lesser wings, the posterior clinoid processes (PC, horizontal arrow in A) projecting forward from the dorsum sellae (DS), and the lateral (L) and the medial (M) pterygoid (P) plates projecting inferiorly. Parasellar foramina include the foramen rotundum (FR), foramen ovale (FO), foramen spinosum (FS), optic canals (OC), superior orbital fissure (SoF), and pterygoid (vidian) canals (Pt C). From anterior to posterior, note the relationships of the crista galli (CG), planum sphenoidale (PS), limbus (L), chiasmatic sulcus (CS), tuberculum sellae (TS), sella turcica (Se), dorsum sellae (DS), and the clivus (Cli). In A, the chiasmatic sulcus lies between the intracranial ends of the two optic canals (OC) laterally, the limbus (paired arrowheads) anteriorly, and the tuberculum sellae (asterisk) behind. It has been left unlabeled to show its full contour. The petrous apices (PA) lie just posterolateral to the clivus and posterior clinoid processes. They display prominent trigeminal impressions (TI) on their anterior surfaces where the fifth cranial nerve (CN V) passes over the petrous apex to reach Meckel’s cave. Also labeled are the perpendicular plate of the ethmoid bone (PPE) and the vomer (Vo), which together form the nasal septum, and the cribriform plate (CP), which overlies the ethmoid labyrinth.
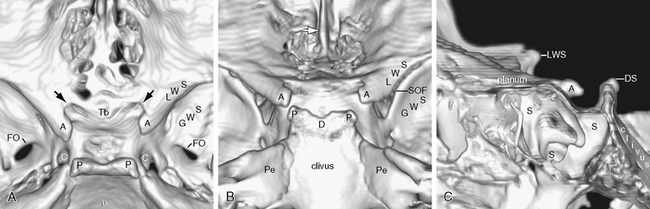
FIGURE 14-2 A to C, Three-dimensional (3D) surface reformatted images of the sella turcica. A, Top view. B, Posterosuperior view. C, Cut-plane midsagittal section of the 3D reformatted image, with anterior to the reader’s left. Compare with the dried bone specimens of Figure 14-1. A, anterior clinoid process; C, carotid groove; D, dorsum sellae; FO, foramen ovale; GWS, greater wing of the sphenoid; LWS, lesser wing of the sphenoid; Pe, petrous apex; S, sphenoid air cells; SOF, superior orbital fissure; Tb, tuberculum sellae. Black arrows show intracranial ends of the optic canals. White arrow in B indicates the crista galli. See www.expertconsult.com for 3D surface-rendered videos of the sella with rotation in the horizontal, vertical, and multiaxial planes, respectively. These renderings provide a frame of reference regarding the spatial relationships of the sella, orbits, and skull base structures described throughout this chapter that are hard to capture on conventional 2D images.
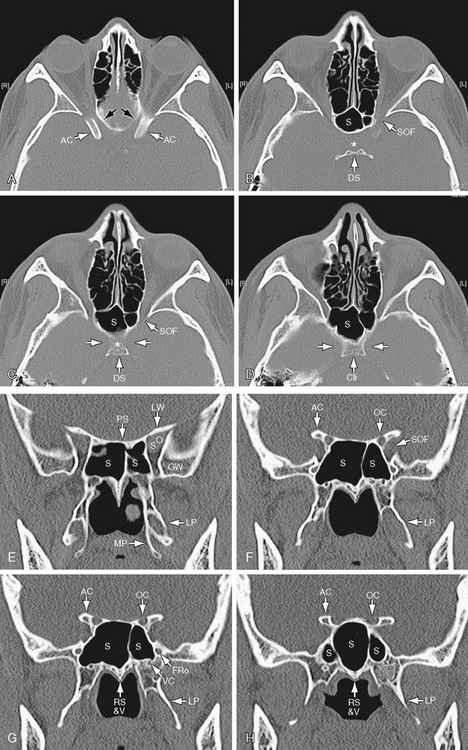
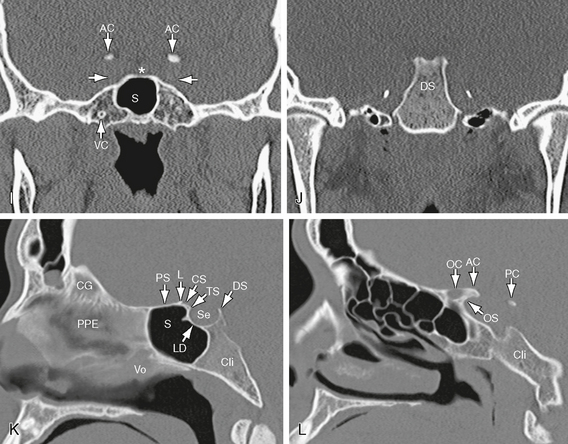
FIGURE 14-3 CT of the sella turcica and parasellar structures—bone algorithm images in axial plane (A to D), coronal reformatted sections (E to J), and sagittal reformatted sections (K to L). A to D, Axial images presented from superior to inferior demonstrate the normal anatomy of the sphenoid bone (S), anterior clinoid (AC) processes, and dorsum sellae (DS). The optic canals (black arrows) align with the optic nerves and pass toward the sella turcica immediately medial to the anterior clinoid processes. In B, the position of the sella turcica is indicated by the asterisk. The posterior clinoid processes form paired projections extending anteriorly from the dorsum. The partially ossified petroclinoid ligaments extend posterolaterally from the dorsum. The superior orbital fissure (SOF) appears to align with the medial walls of the orbit. In C and D, the bony grooves (horizontal white arrows) for the internal carotid arteries mold the lateral contours of the sella. Cli, clivus. E to H, Coronal images displayed from anterior to posterior. The body of the sphenoid contains asymmetric sphenoidal air cells (S) of diverse size. The planum sphenoidale (PS) forms the roof of the sphenoidal sinus anteriorly. The superior orbital fissure (SO) lies between the lesser wing of the sphenoid (LW) above and the greater wing of the sphenoid (GW) below. The anterior clinoid processes (AC) project posteriorly from the medial edges of the lesser wings. The optic canals (OC) lie between the body of sphenoid medially, the optic struts superiorly and inferiorly, and the anterior clinoid processes (AC) laterally. The inferior optic strut separates them from the superior orbital fissure (SOF). The floor of the optic canal extends further posterior than the roof, so sections through its intracranial end of the optic canals (G) show thinning to absence of the roof but a robust floor. The medial (MP) and lateral (LP) pterygoid plates project inferiorly from the body of the sphenoid. The lateral plate is larger and extends further posterior, so it is depicted in multiple adjacent posterior sections. The inferior surface of the sphenoid has a “keel” shape designated the rostrum. The vaginal processes of the vomer insert onto the inferior surface of the rostrum, just to each side of midline. The foramen rotundum passes anteriorly at the side of the sphenoid, so it is always seen best on coronal sections. The vidian canals (pterygoid canals) (VC) pass through the body of the sphenoid just above the pterygoid processes. I and J, Coronal images continued. I, Coronal section through the mid sella turcica (asterisk) shows the thin floor of the sella above the sphenoidal sinus (S), the carotid grooves (white arrows) molding the walls of the sphenoid laterally, and the posteriormost ends of the anterior clinoid processes. J, Immediately posteriorly, the dorsum sellae (DS) forms the posterior wall of the sella turcica. Nubbins of the posterior clinoid processes are seen at the top of the dorsum. Short ossified segments of the petroclinoid ligaments lie laterally. K and L, Sagittal images. K, Midsagittal section shows the crista galli (CG), perpendicular plate of the ethmoid bone (PPE), and the vomer (Vo) anteriorly, and the sphenoid sinus (S) and sella turcica (Se) posteriorly. In order from anterior to posterior, the parasellar bony structures are the planum sphenoidale (PS), limbus (L), chiasmatic sulcus (CS), tuberculum sellae (TS), lamina dura (LD), and the dorsum sellae (DS). The cortical bone of the floor of the sella turcica (lamina dura, LD) is thicker and more easily seen where it overlies the aerated sphenoid sinus. It is thinner and less easily appreciated where it overlies the cancellous basi-sphenoid bone. L, Off midline, parasagittal section shows portions of the anterior (AC) and posterior (PC) clinoid processes, the optic canal (OC), and the optic strut (OS).
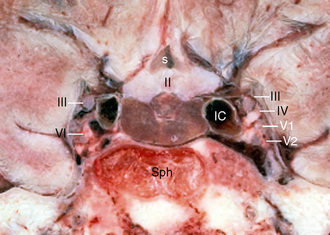
FIGURE 14-4 Gross anatomy of the sella and pituitary gland. Coronal cryomicrotome section through the sella turcica. The sphenoid bone (Sph) forms the bony floor of the sella turcica. The purplish pituitary gland (unlabeled) rests on the floor of the sella between the paired cavernous segments of the internal carotid arteries (IC). The optic chiasm (II) and flask-shaped supraoptic recess (s) of the third ventricle lie above the gland. Cranial nerve VI courses through the cavernous sinus immediately lateral to the internal carotid artery on each side. Cranial nerves III, IV, V1, and V2 course within the lateral wall of the cavernous sinus in strict order from superior to inferior. The deep freezing required for the cryomicrotome technique causes water-containing structures to expand, producing artifactual expansion and crowding of the anatomy.
(Courtesy of Dr. V. M. Haughton, Madison, WI.)
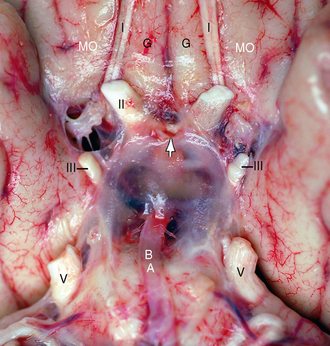
FIGURE 14-5 Gross anatomy of the suprasellar cistern as seen from below with many arachnoid septations preserved. Unfixed anatomic specimen. The olfactory nerves (CN I) (I) pass posteriorly along the olfactory sulci between the paired gyri recti (G) and the paired medial orbital gyri (MO). Arachnoid trabeculae enclose the intracranial ends of the optic nerves (CN II) (II), the oculomotor nerves (CN III) (III) and the trigeminal nerves (CN V) (V). The pituitary stalk (arrow) passes immediately behind the optic chiasm and descends through the trabeculae en route to the neurohypophysis. The basilar artery (BA) ascends along the belly of the pons to enter the suprasellar cistern.
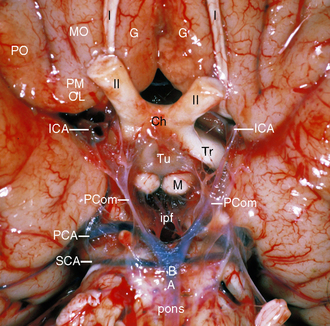
FIGURE 14-6 Gross anatomy of the star-shaped suprasellar cistern as seen from the skull base, looking upward. Unfixed anatomic specimen after partial resection of the arachnoid septations. The paired CN I course along the olfactory sulci between the paired gyri recti (G) medially and the medial orbital gyri (MO) laterally. The posterior orbital gyrus (PO) merges with the medial orbital gyrus (MO) to form the posteromedial orbital lobule (PMOL) that makes up the anterolateral border of the suprasellar cistern on each side. The intracranial segments of the optic nerves (CN II) (II) converge to form the optic chiasm (Ch) in the anterior half of the suprasellar cistern. The optic tracts (Tr) diverge laterally in the posterior half of the suprasellar cistern. The mammillary bodies (M) and tuber cinereum (Tu) form the floor of the hypothalamus just behind the chiasm. The supraclinoid segments of the internal carotid arteries (ICA) lie laterally. The points of the suprasellar star arise where the suprasellar cistern merges into the interhemispheric fissure (anterior point), sylvian fissures (paired anterolateral points), perimesencephalic cistern (paired posterolateral points), and interpeduncular fossa (ipf) (posterior point). Posteriorly, the distal basilar artery (BA) gives rise to the paired superior cerebellar arteries (SCA) and paired posterior cerebral arteries (PCA). The posterior communicating arteries (PCom) pass from the PCAs to the ICAs in the lateral portions of the suprasellar cistern.
The cavernous segments of the internal carotid arteries form paired grooves (carotid sulci) along the lateral surfaces of the upper sphenoid bone. The carotid sulci bulge into the lateral sinus wall in 32% to 71% of patients.5 The bony wall between the carotid artery and the sphenoidal sinus varies from 0.4 to 1.7 mm in thickness and is 0.5 mm or less in approximately 90% of patients (Fig. 14-7). It is absent in 4%, leaving only mucosa between the sinus and the artery.4 The bony wall becomes thinner as one moves anteriorly along the sphenoid and is thinnest in the region of the tuberculum sella.
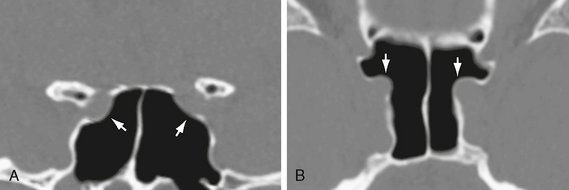
FIGURE 14-7 Thin wall of the carotid groove. Coronal (A) and axial (B) noncontrast CT images through the sphenoidal sinus demonstrate very thin walls between the internal carotid arteries and the aerated sphenoidal sinus (arrows).
The intracarotid distance between the two internal carotid arteries is variable along the course of the cavernous and supraclinoid segments of the artery. In some patients the medial wall of the internal carotid artery (ICA) lies as little as 4 mm from the midline, limiting surgical access. Such medially positioned carotid arteries may flatten or indent the pituitary gland.5
The superior surface of the sphenoidal sinus is a bony plate designated the planum sphenoidale (see Figs. 14-1 to 14-3). Posterior to the planum sphenoidale, the superior surface of the sphenoid bone displays a bony ridge (the limbus), a transverse groove (the chiasmatic sulcus), and a second ridge (the tuberculum sella). The tuberculum sella is the anterior lip of the sella turcica. The contours of these ridges and grooves are always gently rounded, not angular.
The intracranial ends of the optic canals lie at the lateral ends of the chiasmatic sulcus (see Figs. 14-1 to 14-3). The paired anterior clinoid processes form the superolateral margins of the optic canals and give rise to the optic struts that form the lateral walls and floor of each optic canal, separating them from the superior orbital fissure below. The bony wall of the optic canal is less than 5 mm thick in 80% of patients. The wall may be dehiscent, leaving no bony separation between the sinus mucosa and the optic nerve sheath.4
Three bony foramina lie along the floor of the middle cranial fossa medially, at the junction of the body and greater wing of the sphenoid. From anterior to posterior, these are the foramen rotundum (transmitting V2), foramen ovale (transmitting V3), and the foramen spinosum (transmitting the middle meningeal artery). Paired pterygoid (vidian) canals transmit the vidian arteries (arteries of the pterygoid canal) and vidian nerves (nerves of the vidian canal) through the sphenoid bones just where the pterygoid processes arise from the sphenoid body (see Fig. 14-1D and E).
Sphenoidal Sinus
The sphenoidal sinus lies within the body of the sphenoid bone and displays wide variation in size, shape, and degree of pneumatization (Fig. 14-8).6 The sinus is present in rudimentary form at birth as small paired cavities with an intervening septum. The sinus enlarges and expands into the sphenoid bone at least into adolescence and is said to be mature by 14 years of age.6 Nonetheless, some investigators have found that sphenoidal sinus development may continue until the third decade of life.7 The pace of sinus expansion is determined, in part, by the fusion of the sphenoid synchondroses. The adult sphenoid bone forms from multiple individual ossification centers separated by synchondroses. Pneumatization does not cross an intact synchrondrosis, so the sphenoidal sinus does not expand into new portions of the sphenoid until the intervening synchondroses have fused.
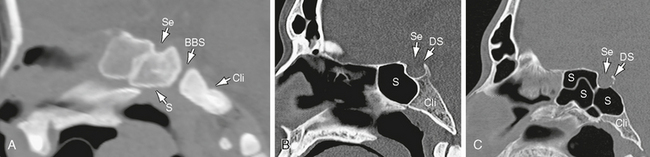
FIGURE 14-8 Sphenoidal sinus aeration. Reformatted midsagittal scan. A, Conchal pattern. This newborn exhibits no aeration of the sphenoid bone (S). The sella turcica (Se) is entirely surrounded by cancellous bone. The basi-sphenoidal/basi-occipital synchondrosis (BBS) separates the basi-sphenoid of the upper clivus from the basi-occiput of the lower clivus (Cli). B, Sellar pattern. Adult with partial pneumatization of the sphenoid bone, reaching to and partially underlying the sellar floor. C, Sellar pattern. Adult with extensive pneumatization of the sphenoid bone extending below the sella and dorsum sellae to reach the posterior cortex of the clivus (Cli). Multiple intrasphenoid septa create air cells of diverse size.
Rhoton4 described three patterns of sphenoidal sinus aeration: conchal, presellar, and sellar (Table 14-1).
1. In the conchal pattern, the sphenoid bone inferior to the sella is formed by solid, nonaerated bone (<2%). The conchal pattern is encountered frequently in children prior to complete sphenoidal sinus pneumatization but is less common in adults.
2. In the presellar pattern (24%), pneumatization stops at the anterior wall of the sella turcica.
3. In the sellar pattern (76%), pneumatization extends below the sella turcica, sometimes as far posteriorly as the clivus (see Fig. 14-8).4,8
TABLE 14-1 Patterns of Sphenoidal Sinus Aeration, Septation, and Grooving
| Pattern | Percentage |
|---|---|
| Conchal type pneumatization | ∼2 |
| Presellar type pneumatization | 21–24 |
| Sellar type pneumatization | 76–78 |
| Sphenoid wing pneumatization | 16 |
| Dorsum sella pneumatization | 14 |
| No major septum | 28 |
| Single major septum | 68 (48 off midline) |
| Two major septa | 4 |
| Septum terminating on carotid groove | 32–40 |
| Carotid artery bulging into sinus | 71 (4% have no bony separation) |
Data from Rhoton AL Jr. The sellar region. Neurosurgery 2002; 51(4 Suppl):S335-S374; Renn WH, Rhoton AL Jr. Microsurgical anatomy of the sellar region. J Neurosurg 1975; 43:288–298; and Hamid O, et al. Anatomic variations of the sphenoid sinus and their impact on trans-sphenoid pituitary surgery. Skull Base 2008; 18:9–15.
Expansion of the sphenoidal sinus laterally into the greater sphenoid wings, either symmetrically or asymmetrically, is designated lateralization (16%).8 Expansion inferiorly into the pterygoid processes and pterygoid plates creates asymmetric pterygoid recesses of the sphenoidal sinus. The sphenoidal sinus may also extend into the vomer, the hard palate, the ethmoid bone, and the basi-occiput, which forms the lower clivus. These variations are generally asymptomatic.9
The degree of pneumatization and the depth of the sphenoidal sinus become important considerations when choosing instrument length for transsphenoidal surgery. During transsphenoidal surgery, the sella turcica appears as a prominent bulge in the roof of the well-aerated sphenoidal sinus. This sellar bulge is an important surgical landmark for the sellar floor.10,11 The sphenoidal sinus depth is defined as the anteroposterior distance from the sphenoidal sinus ostium to the most anterior portion of the sella turcica.4,10 The average depth of the sphenoidal sinus is 15 to 17 mm (range: 11 to 23 mm).4,10 In adults, the instruments used for transsphenoidal surgery must first pass inward along the approach for 11 to 12 cm before encountering the anterior sellar wall. They must then be long enough to reach into the sella and to pass above the sella turcica if additional suprasellar tumor is present.4 In the conchal pattern of sphenoidal sinus aeration, the nonpneumatized sinus is believed to make the transsphenoidal approach less favorable, especially for larger tumors.4,8,12
The septations within the sphenoidal sinus vary widely in size, number, location, orientation, thickness, completeness, and relation to the sellar floor. Sixty-eight to 80 percent of patients show one major septum. The majority of these are situated asymmetrically and may lie several millimeters lateral to the midline. Approximately 28% of patients have no single major septum. Some 4% manifest two major septa. The major sphenoidal sinus septa are typically accompanied by smaller minor septa that may be oriented in any direction, dividing the sinus cavity into multiple smaller cavities. The orientation of these septa and their relationships to the sellar floor and the carotid grooves become important considerations in determining the precise surgical approach to sellar lesions. In 32% to 40% of patients, the major sinus septa terminate on a carotid groove; thus, following the wrong septum at surgery may lead to the artery not the pituitary gland. Further, major septa must be at least partially resected anteriorly to gain access to the sella. Fracture of a septum into the carotid groove may cause inadvertent hemorrhage if such relationships are not identified.5,8,10,13
Sella Turcica and Pituitary Gland
Bony Fossa
The sella turcica has three major components:
1. The tuberculum sella forms the anterior boundary of the sella.
2. The pituitary fossa (hypophysial fossa) is the bony depression that houses the pituitary gland. The floor of the pituitary fossa displays a well-corticated bony wall designated the lamina dura. This lamina is less than 1 mm thick in approximately 82% of cases.5 It is most conspicuous where the sellar floor overlies the aerated sphenoidal sinus and is subtler where the floor overlies cancellous bone.
3. The dorsum sellae forms the posterior wall of the sella. It is continuous inferiorly with the upper portion of the clivus (L., “slope”) that derives from the sphenoid bone (basi-sphenoid).
Sellar Size
The shape and linear dimensions of the sella turcica are highly variable (Fig. 14-9).14 The depth of the sella is measured as the greatest distance perpendicular to a line connecting the tip of the dorsum sellae to the tuberculum sellae. That line corresponds to the plane of the diaphragma sellae. The anteroposterior diameter of the sella has been defined as a line connecting the tuberculum with the farthest portion of the posterior sella wall. Sellar width is defined as the width of the sellar floor between the two carotid sulci. The normal upper limits for these metrics are 17 mm in greatest anteroposterior length, 13 mm in depth, and 15 mm in width. The sellar volume has proved to be a more useful metric than any one linear measure. Total sellar volume is estimated using the equation for the volume of an ellipsoid: 0.5 (length × width × depth in mm)/1000. Total sellar volume should not exceed 1100 mm3.4,5,15
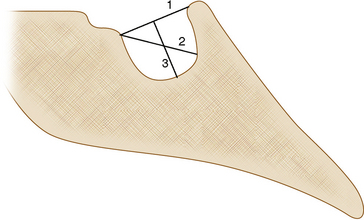
FIGURE 14-9 Schematic representation of measurements made to assess sellar size. Line 1 is drawn from the tuberculum sellae to the tip of the dorsum sellae. Line 2 is the anteroposterior diameter of the sella, which is taken as the line drawn from the tuberculum sellae to the farthest point on the posterior sellar wall. Line 3 indicates the depth of the sella, which is taken as the length of the perpendicular line drawn from line 1 to the deepest portion of the sella turcica.
The length and diameter of the sella turcica increase with age. The growth rate is rapid in the first few years of life, decreases later in childhood, increases again substantially at puberty, and then ceases during late adolescence to early adulthood.14,16,17 The growth rate is greatest during puberty when the pituitary gland undergoes physiologic hypertrophy. Females reach puberty at an earlier age than males, so they show sellar enlargement approximately 2 years earlier than males. After puberty, and into early adulthood, males and females show nearly equal sellar size (except in females during pregnancy).18,19
Clinoid Processes and Dural Reflections/Ligaments
Three pairs of clinoid processes arise in relation to the sella turcica (see Figs. 14-1 to 14-3). Anteriorly, the paired anterior clinoid processes arise from the medial aspects of the lesser sphenoid wings and project laterally to each side of the sella turcica.20 Paired middle clinoid processes form tiny bony elevations along the anterolateral margins of the sellar floor. Posteriorly, the posterior clinoid processes arise at the lateral margins of the dorsum sella and project anteriorly. The transverse distance between the anterior clinoid processes is greater than the transverse distance between the posterior clinoid processes.
The clinoid processes give attachment to important dural reflections (Fig. 14-10) (see also Chapter 8). The free medial margins of the tentorium sweep anteriorly, pass lateral to the posterior clinoid processes, and insert into the anterior clinoid processes on each side. The lateral margins of the tentorium pass medially along the superior petrous ridges, become the petroclinoid ligaments, pass medially below the free margins of the tentorium, and insert into the posterior clinoid processes. The petroclinoid ligaments are the superior margins of the ostia into Meckel’s caves. The cavernous segments of the internal carotid arteries transition into the supraclinoid segments by passing immediately medial to the anterior clinoid processes. They are maintained in position, in part, by the caroticoclinoid ligaments that extend between the anterior and middle clinoid processes to enclose the arteries. The diaphragma sellae is the dural covering of the sella turcica. It merges with the dura of the cavernous sinuses, laterally, and extends farther into the dural folds surrounding the anterior and posterior clinoid processes.3,4,13
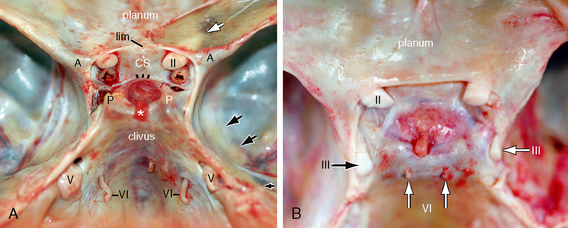
FIGURE 14-10 Gross anatomy of the sellar/parasellar region in situ. Two unfixed cadaver specimens seen from above. A, The dural cover of the right orbital roof has been deflected medially to show the optic canal (white arrow) beneath its thin bony roof. The optic nerves (II) enter the intracranial space medial to the anterior clinoid processes (A) and anterosuperior to the internal carotid arteries. The pituitary gland lies within the sella turcica between the tuberculum sellae (three black dashes) anteriorly and the dorsum sellae posteriorly. The cut end of the pituitary stalk (infundibulum) (asterisk) joins the superior surface of the pituitary gland by passing through the hiatus in the thin glistening diaphagma sellae. The transverse dimension between the two anterior clinoid processes (A-A) is wider than the transverse distance between the two posterior clinoid processes (P-P). The petroclinoid ligaments pass anteromedially from the petrous apices to insert into the posterior clinoid processes, forming the superior margins of the ostia through which the trigeminal nerves (V) enter into Meckel’s cave (black arrows

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


